Alzheimer’s In Young People: Causes, Symptoms And Treatment
Alzheimer’s disease, a neurodegenerative disorder devastating to the life of those who suffer from it and those around them, manifests itself very frequently in old age. However, it’s not always like that. Although it is not so common, can appear before age 65 and even during early adulthood. In fact, the first presentation of the disease is described in the case of a 55-year-old woman.
There are some reasons to believe that late-life Alzheimer’s disease and adult-onset Alzheimer’s disease, although they share many characteristics, could actually be variants of the same clinical entity. How does this disease appear and how can we detect it in time, then?
The objective of the article is not to provide an exhaustive definition of the classic presentation of Alzheimer’s, but it is necessary to refresh your memory and remember what the most characteristic symptoms of Alzheimer’s disease are.
Alzheimer’s in old age
The most common clinical presentation is episodic memory loss, which is accompanied by progressive deterioration of other cognitive domains. such as voluntary movements or the ability to produce and understand language. This definition is not rigid, since many other cases present a focal alteration of only one of the domains without memory impairment. For this reason, when we talk about Alzheimer’s disease we are talking about a very heterogeneous set of presentations that all have the same cause.
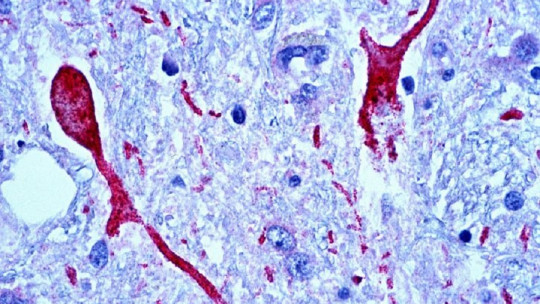
At the brain level, we observed the formation of senile plaques and neurofibrillary tangles. Plaques are nothing more than deposits of peptides that form with aging. It is common to have these plaques even in healthy adults, but we find a greater number of them in patients with Alzheimer’s disease. Neurofibrillary tangles, on the other hand, are hyperphosphorized conglomerates of tau protein. Its presence in the brain is also a predictor of neurocognitive disorder.
About 4% of Alzheimer’s patients are diagnosed before the age of 65. The most common form of Alzheimer’s onset in young age is not through memory loss, but through non-amnestic syndromes. For example, visuospatial dysfunctions, apraxias, anomies, etc. Thus, we will find that executive, visuospatial and motor functions are usually affected in these patients, confusing the diagnosis with other disorders.
At the brain level, like its larger analogues, These patients also have a greater number of senile plaques and neurofibrillary tangles. However, its location is different. In young adults who develop Alzheimer’s disease, the hippocampus is preserved and free of involvement by these deposits. Let us remember that the hippocampus is a cardinal point in the acquisition and retrieval of memory. This finding largely explains the difference in presentations, why in older people memory is affected from the beginning and why in young people with Alzheimer’s this is uncommon.
Neuropathology shows that there is a greater density and more diffuse distribution of the typical signs of Alzheimer’s. Structural neuroimaging studies show that the cortex is more affected than in elderly patients and also more diffusely, especially affecting the neocortex.
Taking all this evidence into account, it is possible to affirm that although both manifestations fall under the label of Alzheimer’s disease because they meet the same diagnostic criteria, the pathological processes suffered by young people are different from those found in older patients. The lesions are distributed differently, so we could be talking about two variants of the same disease, not just a criterion of temporality.
In Alzheimer’s that occurs in old age, the disease occurs due to the formation of natural deposits. The older the patient, the more likely they are to have so many waste deposits that their cognitive abilities begin to worsen. Likewise, each person’s lifestyle may or may not protect the formation of these deposits present in the disease.
However, In normal young patients there is no time for these deposits to form. No normal process justifies such density and pathological distribution in the brain. This is why many cases of Alzheimer’s that begin at an early age occur due to mutations in the genes that allow protein deposits to accumulate and senile plaques to form.
Instances of Alzheimer’s due to mutations that are passed down genetically are rare. It is believed that most cases occur by acquisition, or because the genes involved do not do their job optimally. It seems more the product of a cluster of genetic factors and lifestyles that produce oxidative stress than of a specific gene or marker. Naturally, those people who come from families with a marked history of Alzheimer’s at a young age, if they wish, can undergo a test where a marker of the presence of said genetic mutation or not can be found and know if they will develop the disease.
Treatment and prognosis
The treatment of Alzheimer’s in young people is the same as that prescribed for the elderly, with the advantage that they can carry out more therapeutic activities than the latter. It is very important to maintain activities of daily living as long as possible and not stop doing them because you have been diagnosed. Autonomy and activities allow the individual to retain their cognitive abilities for much longer and the decline is more gradual.
Cognitive stimulation through activities that use brain functions is a good protector against disease progression. It is impossible to get rid of it or stop it, so the goal is to preserve the greatest autonomy and quality of life possible for the longest period of time. It might be a good idea to make plans about how to manage life later when you begin to depend more on others and are unable to deal with issues such as your own finances, legal procedures, a will, or your own will towards certain medical procedures that you may be subject to. one could be submitted later.
The prognosis of Alzheimer’s at an early age is unfavorable. These people deteriorate more rapidly than the elderly and the cognitive decline is more marked and evident. However, it is important to always focus on the skills that the patient retains and that he can still take advantage of and use them for as long as possible.




")

")