Internal Capsule (part Of The Brain) Components And Functions
The internal capsule is a structure of the brain composed of myelinated fibers through which nerve projections pass that go from the cortex to the medulla and subcortical structures, and vice versa.
In this article we explain in more detail what the internal capsule is, what its composition and anatomical structure are, what functions the most important nerve pathways perform and what consequences injuries have in this region of the brain.
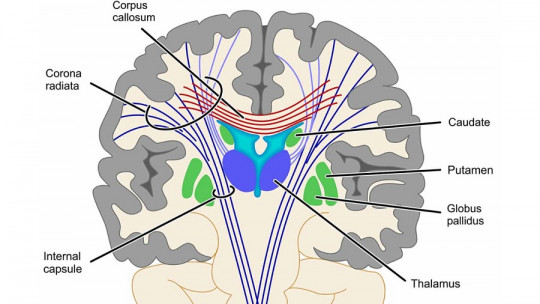
The internal capsule is a region of the brain formed by a small band of myelinated fibers, also called white matter, which separates the lenticular nucleus from the caudate nucleus and the thalamus. This substance is made up of projections that go from the cerebral cortex to different subcortical structures.
This structure It is composed of an anterior arm and a posterior arm, as well as ascending and descending projections Precisely, when these run between the lenticular nucleus and the area of the thalamus and the caudate nucleus, the matter is compacted, giving rise to the internal capsule.
This area of the brain contains vitally important pathways, such as the corticobulbar and corticospinal tracts. In fact, specific lesions in the internal capsule (which can occur, for example, due to cerebrovascular accidents such as heart attacks or strokes) can generate devastating clinical deficiencies for the affected person.
anatomical structure
The internal capsule It does not make up one of the basal ganglia, but rather a bundle of fibers that crosses them The shape of the internal capsule varies depending on how we analyze the brain. If we make a frontal cut, this brain structure takes the shape of an externally open angle with a lower, horizontal side, below the lenticular nucleus.
If we make a horizontal cut, it has a V-shaped appearance, where the knee (its end) points medially, and we can divide it into three fundamental components:
The anterior arm
The anterior arm or lenticulous-caudate portion of the internal capsule separates the lenticular nucleus from the caudate nucleus
It contains fibers that go from the thalamus to the cortex (thalamocortical) and, vice versa, from the cortex to the thalamus (corticothalamic), which join the lateral thalamic nucleus with the cortex of the frontal lobe; to the frontopontine tracts of the frontal lobe with the pontine nucleus; and fibers that run transversely from the caudate nucleus to the putamen.
The posterior arm or lenticulo-thalamic portion of the internal capsule, located between the thalamus and the lenticular nucleus contains essential ascending and descending pathways.
The corticobulbar and corticospinal tracts pass through the anterior half of the posterior arm, with fibers to the face and arm, in front of the fibers to the leg. Corticorubral fibers, which come from the frontal lobe cortex to the red nucleus, accompany the corticospinal tract.
The posterior third of the posterior limb is composed of third-order sensory fibers that go from the posterolateral nucleus of the thalamus to the postcentral gyrus (where the somatosensory cortex, an area of sensory reception, such as touch, is located).
As in the case of the corticospinal and corticobulbar fibers, there is a somatotopic organization of the sensory fibers of the posterior arm, with the face and arm ascending in front of the leg fibers.
Composition of your nerve fibers
The internal capsule is composed of white matter, that is, nerve fibers covered with myelin, a substance that surrounds and protects the axons, allowing for greater speed in the transmission of the nerve impulse.
Depending on the length of the path that each of the fiber bundles travels we can divide these into short and long fibers.
short fibers
This type of fibers link the thalamus with various areas of the cerebral cortex (thalamocortical fibers). They emerge throughout the entire ovoid mass of gray matter that makes up the thalamus and, seen at a macroscopic level, they seem to radiate in all directions (hence the name thalamic radiations).
The anterior thalamic peduncle is composed of fibers that emerge from the anterior part of the thalamus and go to the frontal lobe, occupying the anterior arm of the internal capsule. The superior peduncle, for its part, emerges from the upper and posterior part of the thalamus to go to the parietal lobe, passing through the posterior arm of the internal capsule.
On the other hand, the fibers that connect the posterior area of the thalamus with the occipital lobe they form the posterior peduncle, which also runs along the posterior arm of the internal capsule And finally, the fibers that leave the anterior part of the thalamus and project to the temporal lobe occupy the sublenticular region of the internal capsule and form the inferior peduncle.
This other type of fibers They are responsible for linking the cerebral cortex with nervous areas further away from the brain passing through the internal capsule and occupying the anterior arm, the knee and the posterior arm.
These fibers constitute: the frontopontine fasciculus; the geniculate fasciculus, responsible for voluntary head movements; the pyramidal pathway, responsible for voluntary movements of the trunk and extremities; the sensitive pathway; the parieto-pontine and occipito-pontine fascicles; and the retrolenticular portion or Wernicke’s corridor, an area of great relevance at both a motor and sensory level, and where optical and acoustic radiation intersect.
Features
The internal capsule is a brain region in which two very important nerve fiber tracts converge: the corticospinal tract and the corticobulbar tract Next, we will see what functions each of them fulfills.
The corticospinal tract
The corticospinal tract or pathway is a set of nerve fibers that are part of the internal capsule and They are responsible for controlling voluntary movement of the body It is essential to manage the execution of fine movements (with the fingers of the hand, for example). Its role is to ensure that movements of this type have the appropriate skill and precision.
On the other hand, it also intervenes in the regulation of sensory relays and when selecting the sensory modality that finally reaches the cerebral cortex The corticospinal tract stimulates the neurons responsible for flexion and inhibits those responsible for extension.
In the corticospinal pathway there is a somatotopic representation of the different parts of the body in the primary motor cortex, with each area of the lower limb located in the medial cortex and the area of the cephalic limb located in the lateral cortex, in the convexity of the cerebral hemisphere. (the motor homunculus).
The motor area of the arm and hand is the one that occupies the most space (occupying the precentral gyrus, located between the lower limb area and the face).
The corticobulbar tract
The corticobulbar tract or pathway is a bundle of nerve fibers that is responsible for directing the muscles of the head and neck This nervous tract is responsible for us being able to control, for example, facial expression, or being able to chew or swallow.
The tract arises in the lateral part of the primary motor cortex and its fibers end up converging in the internal capsule of the brainstem. From there, they go to the motor nuclei of the cranial nerves and these connect with the lower motor neurons to innervate the facial and neck muscles.
Consequences of damage to this region of the brain
Lesions in a region of the brain such as the internal capsule can compromise motor and sensory function selectively. For example, lacunar infarcts, strokes less than 15 mm in diameter and caused by the occlusion of the perforating arteries of the brain, can selectively compromise the anterior part of the posterior arm of the internal capsule, producing pure motor hemiparesis.
Lacunar infarctions or strokes can cause another series of symptoms and syndromes, depending on the affected area. Pure sensory syndrome is another of the conditions that occur when infarcts occur located in the internal capsule and/or the posterior nucleus of the thalamus. The affected person, in this case, suffers from facio-brachi-crural hemi-hypoesthesia (reduction of sensitivity in practically half of the body).
Another consequence associated with damage to the cerebral blood vessels, which produces infarction or thrombosis in the posterior arm of the internal capsule, is contralateral hemiplegia (on the opposite side of the body), due to an interruption of the corticospinal fibers that go from the cortex to the spinal cord and the muscles that perform motor functions.
Finally, there are two more disorders that are associated with specific damage to the internal capsule and related structures. On the one hand, dysarthria-clumsy hand syndrome, due to damage to the internal capsule of the knee and which causes symptoms such as facial weakness, manual clumsiness, dysphagia and dysarthria; and on the other hand, paresis with hemiataxia, when the cortico-ponto-cerebellar pathway and the posterior arm of the internal capsule are affected, and which causes symptoms such as paralysis and incoordination of the leg or arm.
I’m Emily Williams Jones, a psychologist specializing in mental health with a focus on cognitive-behavioral therapy (CBT) and mindfulness. With a Ph.D. in psychology, my career has spanned research, clinical practice and private counseling. I’m dedicated to helping individuals overcome anxiety, depression and trauma by offering a personalized, evidence-based approach that combines the latest research with compassionate care.