Deep beneath the surface of your brain, hidden from view like a secret island in a neural archipelago, lies one of the most fascinating and least understood regions of the human cerebral cortex. The insular cortex—often simply called the insula—remained largely mysterious to neuroscientists for decades, not because it’s unimportant, but because it’s buried so deep within the brain’s folds that studying it has always been technically challenging. You can’t see it when looking at a brain from the outside. You have to pull back other brain tissue to reveal it, like opening curtains to discover a hidden room.
What makes this hidden region so intriguing is the staggering range of functions it orchestrates. The insula appears to be involved in nearly everything that makes you feel human: your awareness of your own body’s internal states, your emotional experiences, your ability to feel empathy, your perception of pain, your sense of taste, your capacity for self-awareness, even your understanding of time. It’s been called the brain’s integration hub, a place where information from your body and your environment converges to create your subjective experience of being alive and conscious. When neuroscientist Antonio Damasio studies consciousness and emotion, when researchers investigate addiction or anxiety, when surgeons carefully navigate brain tumors—the insula is there, playing a critical role.
Yet for something so fundamentally important, the Island of Reil—as it’s sometimes called after the German physician who first described it in 1809—receives surprisingly little attention compared to flashier brain regions like the prefrontal cortex or hippocampus. Perhaps this is because the insula doesn’t fit neatly into simple categories. It’s not purely sensory or motor. It’s not exclusively emotional or cognitive. Instead, it seems to exist at the intersection of multiple systems, translating between your body and your mind, between feeling and thinking, between self and world. This integration makes it essential but also difficult to study and understand.
Recent advances in neuroimaging technology have finally begun revealing the insula’s secrets. Functional MRI studies show it lighting up during everything from tasting food to feeling disgusted, from experiencing physical pain to feeling social rejection, from becoming aware of your heartbeat to recognizing your own face. Damage to the insula can have profound effects: people may lose the ability to feel disgust, struggle to identify their emotions, or even lose awareness that they have certain medical conditions. Some individuals with insular damage stop craving cigarettes immediately, suggesting the region plays a crucial role in addiction. These clinical observations confirm what imaging studies suggest—the insula is fundamental to human experience.
Understanding the insula matters not just for neuroscience, but for making sense of human psychology, emotion, and consciousness. It helps explain why emotional and physical pain activate similar brain regions, why mindfulness practices that increase body awareness can reduce anxiety, why certain neurological conditions affect both physical sensation and emotional processing, and how our subjective feelings arise from objective physiological states. Whether you’re a student learning neuroanatomy, a clinician treating neurological or psychiatric conditions, or simply someone curious about how your brain creates your experience of being you, the insula offers profound insights into the biological basis of human consciousness and feeling.
Location and Anatomical Position
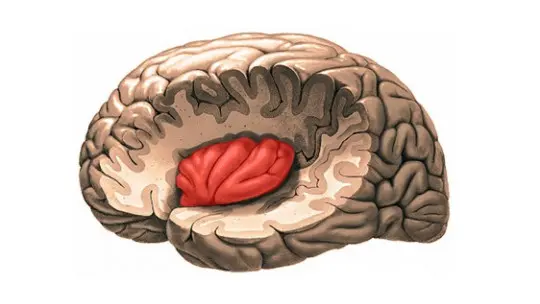
The insula occupies one of the most protected positions in the entire brain. Located deep within the lateral sulcus—also called the Sylvian fissure—this region sits at the floor of a deep groove that runs along the sides of each brain hemisphere. The lateral sulcus is one of the brain’s most prominent anatomical landmarks, separating the temporal lobe below from the frontal and parietal lobes above. Think of it as a deep valley with the insula forming the valley floor, hidden from surface view.
To actually see the insula during a brain dissection or surgery, you must pull back or remove portions of the surrounding lobes. These overlying sections are called the opercula, which literally means “little lids” in Latin—the frontal, parietal, and temporal opercula cover the insula like protective flaps. The frontal operculum includes parts of the inferior frontal gyrus, the parietal operculum contains portions of the postcentral gyrus and inferior parietal lobule, and the temporal operculum consists of the superior temporal gyrus. Only by retracting these opercula can the insular surface be visualized.
The insula’s depth varies across its extent. The insular apex, which is the most superior point, sits approximately 18 millimeters deep from the cortical surface—nearly three-quarters of an inch beneath the brain’s outer layer. At its deepest point near the base, called the limen insulae, the tissue extends an additional 17 millimeters deeper still, making it one of the most buried regions of cortex. This deep position places the insula in close proximity to several critical structures including the extreme capsule, claustrum, external capsule, and putamen as you move from lateral to medial.
The insula is present bilaterally, meaning both the left and right hemispheres contain this structure. However, the two sides aren’t identical. Research using diffusion tensor imaging has revealed that connection patterns differ between left and right insula, with the left hemisphere’s insula showing particularly strong connections to language areas. This anatomical asymmetry likely contributes to functional differences, with the left insula often more involved in language and temporal processing while the right insula plays larger roles in emotional awareness and bodily sensation.
Perhaps the most distinctive anatomical feature defining the insula is the circular sulcus, also called the sulcus of Reil. This semicircular groove completely surrounds the insula, demarcating it from the adjacent opercula and essentially creating an island of cortex—hence the name insula, which means island in Latin. Within this island, several gyri and sulci create the insula’s internal landscape, dividing it into functional subregions that we’ll explore next.
Structural Divisions and Parts of the Insula
The insula isn’t a uniform structure but rather a complex region with distinct subparts that differ in their cellular architecture, connections, and functions. The primary division separates the insula into anterior and posterior sections, demarcated by the central insular sulcus which runs roughly diagonally across the insular surface. This isn’t just an arbitrary anatomical division—the anterior and posterior insula have fundamentally different cellular structures and serve different roles in brain function.
The anterior insula contains three short gyri stacked roughly parallel to each other. From front to back, these are called the anterior short insular gyrus, middle short insular gyrus, and posterior short insular gyrus. These three gyri are separated by two sulci called the precentral insular sulci. The cellular structure of the anterior insula is described as agranular, meaning it lacks the prominent granular cell layer (layer IV) that characterizes primary sensory cortex. This agranular architecture is similar to motor and premotor cortex, suggesting the anterior insula plays more active, output-oriented roles rather than purely receiving sensory information.
The posterior insula consists of two long gyri that run perpendicular to the short gyri of the anterior section. These are the anterior long insular gyrus and the posterior long insular gyrus, separated by a single postcentral insular sulcus. Unlike its anterior counterpart, the posterior insula has granular cytoarchitecture, more resembling primary sensory cortex with its prominent layer IV. This structural difference reflects functional specialization, with the posterior insula more involved in processing sensory information from the body.
Depending on which classification system researchers use, the insula can be subdivided into anywhere from 2 to 13 distinct areas based on differences in cellular architecture, connection patterns, and function. More detailed parcellation schemes identify regions like the parainsular cortex, granular insula, frontal opercular areas, middle insular area, anterior ventral insular area, and anterior agranular insular complex. While these detailed subdivisions matter for research, the fundamental anterior-posterior division captures the most important functional distinction.
| Insular Region | Key Structural Features |
| Anterior Insula | Three short gyri; agranular cytoarchitecture; contains von Economo neurons |
| Posterior Insula | Two long gyri; granular cytoarchitecture; resembles sensory cortex |
| Accessory Gyrus | Located on anterior face; connects to orbital frontal regions |
| Limen Insulae | Anteroinferior apex; where temporal lobe and insula meet |
One of the most intriguing cellular features of the anterior insula is the presence of von Economo neurons, also called spindle neurons due to their distinctive elongated shape. These large, spindle-shaped cells are found in layer V of the anterior insular cortex and are remarkably rare in the animal kingdom—they appear only in humans, great apes, elephants, and some cetaceans, all species known for complex social behavior and high intelligence. Von Economo neurons have large-diameter axons that allow for rapid, long-range communication across brain regions, suggesting they facilitate fast integration of information from diverse sources. Their presence in the anterior insula may explain this region’s role in rapid intuitive judgments and emotional awareness.
Additional smaller structures complete the insular landscape. The accessory gyrus sits on the anterior face of the insula, while the transverse gyrus connects the insula to the orbital surface of the frontal lobe. The limen insulae, located at the anteroinferior apex where the insula meets the temporal lobe and anterior perforated substance, serves as an important surgical landmark because the middle cerebral artery typically bifurcates at this location. Understanding these anatomical details matters tremendously for neurosurgeons attempting to remove tumors or treat epilepsy originating in insular regions, as the insula is surrounded by highly eloquent cortex and critical blood vessels.
Neural Connections and Network Integration
What makes the insula so functionally diverse is its extraordinarily rich pattern of connections to other brain regions. The insula serves as a major integration hub, receiving input from and sending output to an impressive array of cortical and subcortical structures. These connections allow the insula to serve as a translator between different types of information—bodily sensations and emotions, external perceptions and internal states, autonomic arousal and conscious awareness.
The anterior insula maintains particularly strong connections with limbic system structures involved in emotion. It connects extensively to the amygdala, which processes emotional significance and fear responses; the anterior cingulate cortex, involved in emotional regulation and decision-making; the orbitofrontal cortex, which evaluates reward and punishment; and the ventromedial prefrontal cortex, essential for emotional decision-making and self-referential processing. These limbic connections allow the anterior insula to participate in emotional processing and the integration of emotion with bodily states.
The posterior insula has different connection patterns reflecting its more sensory nature. It receives strong input from somatosensory cortex, particularly secondary somatosensory areas that process touch, temperature, and pain. It also connects to the thalamus, the brain’s sensory relay station, receiving information about the body’s internal state. These connections position the posterior insula to monitor and represent bodily sensations, creating what neuroscientists call interoceptive awareness—the sense of the body’s internal condition.
Both anterior and posterior insula maintain connections with the prefrontal cortex, though to different prefrontal regions. The anterior insula connects more to ventral and orbital prefrontal areas involved in emotion and motivation, while the posterior insula connects more to dorsolateral prefrontal regions involved in attention and cognitive control. These prefrontal connections allow insular information about bodily and emotional states to influence higher-order thinking, planning, and decision-making.
The insula also connects extensively with autonomic control regions in the brainstem and hypothalamus. These connections allow the insula to both monitor and influence autonomic functions like heart rate, blood pressure, digestion, and respiration. When you become consciously aware of your racing heart during anxiety, that awareness likely involves insular processing of autonomic information. When meditation practices that increase insular activation lead to better autonomic regulation, these connections are the pathway.
Modern neuroimaging has revealed that the insula participates in several large-scale brain networks. It’s a core node in the salience network, which identifies stimuli that deserve attention and coordinates appropriate responses. The salience network, anchored by the anterior insula and anterior cingulate cortex, acts like a switch that determines whether the brain should engage task-focused attention or self-referential thinking. The insula’s central position in this network explains why it activates during such diverse experiences—it’s fundamentally involved in detecting what matters and coordinating responses.
Functions of the Insular Cortex
Given its complex structure and extensive connections, it’s perhaps unsurprising that the insula participates in an remarkably wide range of functions. Rather than serving a single specific purpose, the insula integrates multiple types of information to create rich, multimodal representations that support consciousness and subjective experience. Let’s explore the insula’s major functional roles.
Interoceptive awareness represents perhaps the insula’s most fundamental function. Interoception refers to the sense of your body’s internal state—your heartbeat, breathing, stomach sensations, muscle tension, temperature, itch, hunger, thirst, and all the subtle signals your body constantly generates. The insula, particularly the posterior portion, receives and processes this interoceptive information, creating a neural representation of how your body feels. Studies show that people with greater insular activation during interoceptive tasks have better accuracy at detecting their own heartbeat, and that practices like mindfulness meditation that increase body awareness show corresponding changes in insular activity and structure.
Emotional processing and awareness relies heavily on the anterior insula. Antonio Damasio’s somatic marker hypothesis proposes that emotions involve bodily changes that are then represented in the brain to create feelings. The insula serves as a critical link in this process, integrating information about bodily changes with contextual information to generate emotional experiences. Neuroimaging studies consistently show insular activation during virtually every emotional state studied—happiness, sadness, anger, fear, disgust, and more. Damage to the insula can impair emotional awareness, with patients showing difficulty identifying and describing their own emotional states, a condition called alexithymia.
Pain perception involves the insula as a key component of the pain matrix. While the primary somatosensory cortex processes the location and intensity of painful stimuli, the insula contributes the suffering and emotional aspects of pain—the unpleasantness that makes pain aversive. This explains why the insula activates not just during physical pain but also during social pain like rejection or exclusion. The brain appears to process social and physical pain through overlapping systems, with the insula playing a central role in both. Chronic pain conditions often show altered insular structure and function, suggesting this region’s involvement in both acute pain processing and the transition to chronic pain states.
Disgust appears to have particularly strong representation in the anterior insula. Studies using facial expressions show that viewing disgusted faces activates the insula more than any other emotion, and people with insular damage show impaired recognition of disgust in others and reduced experience of disgust themselves. The connection between disgust and the insula makes evolutionary sense—disgust originally evolved to prevent consumption of contaminated food, which would involve interoceptive signals like nausea. The insula’s role in monitoring bodily states positions it perfectly to process this aversive emotion. Interestingly, moral disgust—the feeling of revulsion toward ethical violations—also activates the insula, suggesting the brain co-opted physical disgust mechanisms for social and moral judgments.
Taste perception involves the primary gustatory cortex, which is located in the insula. When you taste food, signals from taste receptors travel through brainstem nuclei to the thalamus and then to the insula, creating the conscious experience of taste. The insula integrates taste information with other relevant signals—smell, texture, temperature, context, past experiences—to create rich flavor experiences. Damage to the insula can impair taste perception, while insular tumors sometimes present with taste disturbances as an early symptom.
Self-awareness and consciousness may depend fundamentally on insular function. The insula’s integration of bodily signals, emotional states, and contextual information creates a moment-to-moment sense of self and current experience. The presence of von Economo neurons only in species with demonstrated self-recognition and complex social behavior suggests these specialized insular cells may contribute to sophisticated self-awareness. Studies of meditation practices that increase present-moment awareness show corresponding changes in insular structure and connectivity. Some neuroscientists propose that consciousness itself emerges from the brain’s representation of bodily states, with the insula playing a starring role in this process.
Empathy and social cognition involve the insula’s ability to simulate others’ experiences. When you observe someone else in pain, your insula activates in patterns similar to when you experience pain yourself, creating a neural basis for empathy. The anterior insula shows particular activation during empathic responses, moral decision-making, fairness considerations, and processing social exclusion. People with greater insular gray matter volume show higher empathy scores on questionnaires, while conditions like psychopathy that involve empathy deficits show altered insular function.
Addiction and craving involve insular circuits in profound ways. The insula appears to generate the subjective urge to use substances, with neuroimaging showing strong insular activation when addicted individuals are exposed to drug-related cues. Remarkably, case studies of smokers who suffered insular strokes found that many immediately lost all desire to smoke without withdrawal symptoms—their addiction simply vanished. This suggests the insula is necessary for maintaining conscious urges to use substances, making it a potential target for addiction treatments.
Time perception has been linked to insular function, with studies suggesting the insula helps create the subjective sense of time’s passage. The insular accumulation and integration of interoceptive signals may provide the stream of changing bodily states that we experience as time flowing. Conditions that alter insular function, including certain medications and meditation practices, can correspondingly alter time perception.
Clinical Significance and Pathology
The insula’s involvement in such diverse functions means that insular pathology can produce wide-ranging symptoms affecting physical sensation, emotion, cognition, and behavior. Understanding insular dysfunction helps explain numerous neurological and psychiatric conditions while also highlighting this region’s importance in normal brain function.
Insular strokes, while relatively uncommon, produce distinctive symptom patterns. Because the middle cerebral artery supplies the insula, vascular events affecting this vessel can damage insular tissue. Patients may experience disturbances in taste, altered pain perception, difficulty identifying emotions, changes in autonomic regulation, or the sudden disappearance of addiction cravings mentioned earlier. Some insular stroke patients develop a condition where they’re unaware of their neurological deficits—they might be paralyzed on one side but insist nothing is wrong, a phenomenon called anosognosia that demonstrates the insula’s role in self-awareness.
Insular gliomas (brain tumors) present particular surgical challenges. The insula’s deep location surrounded by eloquent cortex, proximity to critical blood vessels, and involvement in language in the dominant hemisphere make insular surgery technically demanding and risky. However, insular tumors also produce distinctive symptoms that can aid diagnosis: taste disturbances, unusual sensory experiences, emotional changes, or seizures with autonomic features like changes in heart rate or breathing. Surgical approaches to the insula must carefully navigate surrounding structures, with outcomes depending heavily on preserving nearby eloquent cortex and vascular structures.
Epilepsy originating in the insula produces seizures with characteristic features. Insular epilepsy often involves prominent autonomic symptoms—changes in heart rate, breathing, sweating, or gastrointestinal sensations—along with emotional experiences like fear or unusual bodily sensations. These seizures can be difficult to diagnose because the symptoms are so different from typical seizures, and the insula’s deep location makes it challenging to identify as the seizure origin on scalp EEG recordings. Some patients with intractable insular epilepsy benefit from surgical removal of the affected tissue if the seizure focus can be precisely localized.
Anxiety disorders consistently show altered insular structure and function. Studies using functional MRI reveal that anxious individuals show heightened insular activation in response to uncertain or threatening stimuli, excessive attention to bodily sensations, and altered connectivity between the insula and emotion regulation regions. This makes sense given the insula’s role in processing bodily signals and generating awareness of physiological arousal. The insula may contribute to anxiety by amplifying normal bodily sensations into symptoms that feel threatening, creating a vicious cycle where increased attention to bodily states generates more anxiety, which produces more bodily changes to attend to.
Depression involves insular abnormalities in both structure and function. Depressed individuals often show reduced insular volume and altered activation patterns during emotional processing. The insula’s involvement in generating feelings from bodily states may explain somatic symptoms of depression like fatigue, appetite changes, and physical pain. Some researchers propose that depression involves a fundamental disturbance in how the brain represents bodily and emotional states, with insular dysfunction playing a central role.
Autism spectrum disorder shows distinctive insular differences. Individuals with autism often have altered insular structure and connectivity, particularly in circuits connecting the insula to social cognition regions. Given the insula’s roles in empathy, emotional awareness, and integrating information from multiple sources, these differences may contribute to social and sensory symptoms. Some researchers suggest that altered insular processing of bodily signals could explain difficulties with emotional awareness and regulation seen in autism.
Chronic pain conditions involve persistent changes in insular structure and function. Patients with fibromyalgia, chronic back pain, irritable bowel syndrome, and other chronic pain syndromes show altered insular activation patterns and changes in insular gray matter. The insula’s central role in pain’s emotional and suffering components means that insular dysfunction can maintain pain even when the original injury has healed, contributing to chronic pain’s persistence.
Research Methods and Studying the Insula
Studying the insula presents unique challenges due to its deep location and complex connectivity. Researchers have developed several complementary approaches to understand this hidden region’s structure and function, each with particular strengths and limitations.
Functional magnetic resonance imaging (fMRI) has revolutionized insular research by allowing non-invasive visualization of insular activation during various tasks and experiences. By measuring blood flow changes that reflect neural activity, fMRI reveals which brain regions activate during pain, emotion, taste, interoception, decision-making, and countless other processes. Studies consistently showing insular activation across diverse experiences helped establish its role as an integration hub. However, fMRI has limitations: it measures indirect correlates of neural activity rather than activity itself, its temporal resolution is relatively poor, and the insula’s proximity to air-filled sinuses can create artifact that complicates imaging.
Diffusion tensor imaging (DTI) maps white matter tracts by measuring water diffusion in brain tissue. This technique has revealed the insula’s extensive connections to other regions, showing how anterior and posterior insula have different connection patterns, how left and right insula differ in connectivity, and how insular connections change with development, aging, and disease. DTI has been crucial for understanding the insula’s position within larger brain networks.
Lesion studies examining patients with insular damage from strokes, tumors, or surgical removal provide some of the strongest evidence about insular function. When the insula is damaged, researchers can observe what capabilities are lost or altered, providing causal evidence that the insula is necessary for those functions. The famous cases of smokers losing addiction after insular strokes came from lesion studies. However, lesion studies have limitations: damage is rarely confined precisely to the insula, patient numbers are often small, and the brain’s plasticity means function may reorganize after damage.
Intracranial recording during epilepsy surgery provides the highest-resolution data about insular function. Patients undergoing evaluation for epilepsy surgery sometimes have electrodes placed in or near the insula to localize seizure origins. Researchers can record directly from insular neurons during various tasks, providing precise temporal and spatial information impossible to obtain non-invasively. However, these studies involve patients with epilepsy whose brains may not represent typical function, and opportunities for such recording are limited.
Animal studies allow experimental manipulations impossible in humans, but interpreting insular research in other species requires caution. Many of the insula’s most sophisticated functions—complex emotional awareness, self-consciousness, abstract empathy—may be unique to humans or greatly elaborated compared to other species. The presence of von Economo neurons only in highly intelligent species suggests some insular functions may not be well-conserved across evolution. Nevertheless, animal studies have provided valuable information about insular connections and basic sensory functions.
FAQs About the Cerebral Insula
Can you live without your insula or with damage to it?
Yes, people can survive with insular damage, though the effects depend on the extent and location of injury. Small insular lesions from strokes or limited surgical removal may produce relatively subtle changes that don’t dramatically impair daily functioning. However, extensive bilateral damage to the insula would likely have profound effects on emotional awareness, pain perception, bodily sensation, and potentially consciousness itself. Case studies of patients with insular damage reveal diverse symptoms: some lose the ability to recognize disgust in themselves or others, some experience altered pain sensitivity, and some show reduced awareness of their own emotions (alexithymia). The famous smokers who lost their addiction after insular strokes demonstrates one dramatic effect of damage. Importantly, the brain shows remarkable plasticity, so function may partially reorganize after insular injury, particularly if damage occurs gradually or early in development. People with insular damage typically require careful monitoring for autonomic dysfunction, seizures, and changes in emotional or sensory processing that might affect safety and quality of life.
What is the difference between the anterior and posterior insula?
The anterior and posterior insula differ fundamentally in structure, connections, and function, representing a key organizational principle of this brain region. Structurally, the anterior insula has agranular cytoarchitecture (lacking prominent layer IV granule cells) and contains specialized von Economo neurons, while the posterior insula has granular architecture resembling sensory cortex. In terms of connections, the anterior insula links extensively to limbic and emotional regions like the amygdala, anterior cingulate, and orbitofrontal cortex, while the posterior insula connects more to somatosensory areas and the thalamus. Functionally, this translates to the posterior insula primarily processing bodily sensations and interoceptive signals—the “raw data” about your body’s state—while the anterior insula integrates this information with emotional and contextual signals to create subjective feelings and awareness. Think of the posterior insula as sensing and the anterior insula as feeling and interpreting. Research shows different activation patterns: the posterior insula responds more to actual changes in bodily state, while the anterior insula activates more during attention to those states and their emotional significance. Understanding this anterior-posterior distinction helps explain the insula’s diverse functions and guides clinical interpretation of insular pathology.
Why is the insula called the Island of Reil?
The name “Island of Reil” honors Johann Christian Reil, the German physician, anatomist, and psychiatrist who first described the insular cortex in detail in 1809. Reil identified this region as a distinct cortical area hidden beneath the overlying frontal, parietal, and temporal lobes. The “island” metaphor is particularly apt because the insula is completely surrounded by the circular sulcus (sulcus of Reil), which separates it from adjacent cortex like water surrounding an island. When you open the lateral sulcus and retract the opercula, the insula emerges as an island of cortex nestled deep within the brain’s geography. The name “insula” itself is Latin for island, making “Island of Reil” somewhat redundant but emphasizing both the anatomical configuration and its discoverer. While modern neuroscientists typically use “insula” or “insular cortex,” the term Island of Reil persists in medical and anatomical literature, connecting contemporary understanding to this region’s discovery over 200 years ago. Reil made numerous contributions to neuroanatomy and psychiatry, but his identification of the insula remains his most lasting legacy in neuroscience.
How does the insula relate to mindfulness and meditation?
The insula and mindfulness practices share an intimate relationship that’s been extensively documented in neuroscience research. Mindfulness meditation typically involves sustained attention to present-moment experience, particularly bodily sensations, breathing, and internal states—exactly the interoceptive information that the insula processes. Studies consistently show that experienced meditators have increased gray matter volume in the insula compared to non-meditators, with the degree of structural difference correlating with years of practice. Functional imaging during meditation reveals heightened insular activation, particularly in the anterior insula, suggesting enhanced processing of bodily states and present-moment awareness. This makes mechanistic sense: meditation involves deliberately attending to the subtle bodily sensations that the insula represents, essentially exercising and strengthening insular circuits through repeated practice. The benefits of mindfulness for anxiety, depression, and chronic pain may work partly through enhanced insular function—better interoceptive awareness allows earlier detection of rising distress and more effective emotion regulation. Some researchers propose that meditation’s effects on consciousness and self-awareness result from changes in how the insula integrates information from body and environment. Importantly, even brief mindfulness training can alter insular structure and function, suggesting these changes don’t require decades of practice. The insula provides a neural mechanism for understanding how attention to bodily experience can transform mental health and wellbeing.
What role does the insula play in addiction?
The insula’s role in addiction has emerged as one of the most exciting discoveries in addiction neuroscience. The insula appears to generate the conscious urge or craving to use substances—that subjective feeling of wanting drugs, alcohol, or cigarettes that drives addictive behavior. Neuroimaging studies show strong insular activation when addicted individuals view drug-related cues, anticipate drug use, or experience withdrawal. The anterior insula particularly lights up during craving states across various addictions. The most dramatic evidence comes from case studies of smokers who suffered insular strokes: a significant proportion immediately lost all desire to smoke without experiencing withdrawal symptoms or effortful quitting. Their addiction simply vanished, suggesting the intact insula is necessary for maintaining conscious drug cravings. This finding has sparked interest in the insula as a potential therapeutic target—if insular function could be temporarily disrupted or modified, might addictions lose their grip? The insula likely contributes to addiction by integrating bodily signals associated with drug use or withdrawal (processed in posterior insula) with emotional and motivational information (processed in anterior insula) to generate conscious craving. Its connections to reward circuitry, prefrontal decision-making regions, and autonomic control areas position it perfectly to translate unconscious drug-related processes into conscious urges that drive behavior. Understanding insular mechanisms in addiction opens new avenues for treatment, potentially through targeted brain stimulation, medications affecting insular circuits, or psychological interventions that modify insular responses to triggers.
Can insular dysfunction cause mental health problems?
Yes, insular dysfunction is implicated in numerous mental health conditions and likely contributes causally to psychiatric symptoms rather than being merely a consequence. The insula’s central role in processing bodily signals, generating emotional awareness, and integrating internal and external information means that when it malfunctions, subjective experience becomes disturbed in profound ways. In anxiety disorders, the insula shows hyperactivation and altered connectivity, possibly amplifying normal bodily sensations into symptoms that feel threatening and generating excessive worry about bodily states. This could create anxiety’s characteristic vicious cycles where attention to physical symptoms increases distress, which produces more symptoms to worry about. In depression, reduced insular volume and abnormal activation patterns may contribute to emotional numbing, difficulty experiencing pleasure, and the somatic symptoms like fatigue and pain that often accompany mood disturbances. Post-traumatic stress disorder shows altered insular responses to trauma-related cues, potentially contributing to intrusive bodily memories and hyperarousal. Autism spectrum disorder involves distinctive insular differences that may relate to difficulties with emotional awareness and social cognition. Even conditions like eating disorders show insular abnormalities that might distort awareness of hunger, fullness, and bodily states. Importantly, many psychiatric treatments—medications, therapy, mindfulness—produce changes in insular structure and function, suggesting that therapeutic benefit partly involves normalizing insular processing. Understanding the insula’s role in mental health opens possibilities for targeted interventions, whether through brain stimulation, medications affecting insular circuits, or psychological approaches that modify how the insula processes information. The insula may be where mind and body meet in both health and illness.
Use this citation format to reference the article clearly and help readers find the original source.
PsychologyFor. (2025). Cerebral Insula: What it Is, Location, Parts and Functions. PsychologyFor. https://psychologyfor.com/cerebral-insula-what-it-is-location-parts-and-functions/
