
Some children seem to move through the world on a different frequency — not broken, not less, but genuinely different in how their brain processes information, regulates attention, coordinates movement, or makes sense of social signals. Neurodevelopmental disorders are conditions that arise from differences in how the brain develops during the prenatal period and early childhood, producing characteristic patterns of cognitive, communicative, behavioral, or motor difficulty that typically become apparent before a child enters school — and that shape how a person experiences the world across their entire lifespan.
These are not conditions that appear suddenly or are caused by poor parenting, trauma, or personal failing. They are neurobiological in origin, rooted in the complex interplay of genetics, epigenetics, prenatal environment, and early neural development. And they are far more common than most people realize. Taken together, neurodevelopmental disorders affect between 10% and 15% of children globally, making them among the most prevalent groups of conditions in developmental medicine and child psychology.
The range is enormous. Neurodevelopmental disorders include conditions as varied as autism spectrum disorder, ADHD, dyslexia, intellectual disability, Tourette syndrome, cerebral palsy, and developmental coordination disorder — each with its own profile of strengths and challenges, its own neurobiological underpinnings, and its own optimal approaches to support and intervention. What they share is their origin in development itself: the brain during its most formative period.
Understanding the different types of neurodevelopmental disorders matters enormously — for parents navigating a new diagnosis, for educators designing inclusive classrooms, for clinicians building assessment and intervention plans, and for the millions of neurodivergent adults seeking language and frameworks for their own lived experience. This article provides a comprehensive, evidence-based guide to each major category, its defining features, and what support looks like in practice.
What Are Neurodevelopmental Disorders? Definition and Key Characteristics
Neurodevelopmental disorders are a group of conditions originating in the developmental period — typically apparent from early childhood — that involve deficits in personal, social, academic, or occupational functioning arising from disruptions in the typical development of the brain and central nervous system. The term encompasses a wide range of presentations, from highly specific learning difficulties to pervasive impairments affecting nearly every domain of daily life.
The DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition) classifies neurodevelopmental disorders into six primary categories:
- Intellectual developmental disorders (intellectual disability and global developmental delay)
- Communication disorders (language disorder, speech sound disorder, childhood-onset fluency disorder, social communication disorder)
- Autism spectrum disorder (ASD)
- Attention-deficit/hyperactivity disorder (ADHD)
- Specific learning disorders (affecting reading, writing, or mathematics)
- Neurodevelopmental motor disorders (developmental coordination disorder, stereotypic movement disorder, tic disorders)

Several important features characterize this group as a whole:
- Early onset: deficits emerge during the developmental period, typically before or during primary school age
- Neurobiological basis: all are presumed to have neurobiological origins, involving genetic, epigenetic, and environmental factors affecting brain development
- Lifelong course: while severity and functional impact may change significantly with development and intervention, neurodevelopmental disorders are generally lifelong profiles rather than transient conditions
- High comorbidity: co-occurrence of multiple neurodevelopmental disorders is the rule rather than the exception — ADHD and dyslexia frequently co-occur, ASD commonly presents alongside ADHD and anxiety, and intellectual disability often accompanies other disorders
| DSM-5 Category | Key Examples |
|---|---|
| Intellectual developmental disorders | Intellectual disability, global developmental delay |
| Communication disorders | Language disorder (DLD), stuttering, social communication disorder |
| Autism spectrum disorder | ASD (all former subtypes) |
| ADHD | Inattentive, hyperactive-impulsive, combined presentations |
| Specific learning disorders | Dyslexia, dyscalculia, dysgraphia |
| Motor disorders | DCD, Tourette syndrome, stereotypic movement disorder |
Intellectual Disability: When Cognitive Development Follows a Different Path
Intellectual disability (ID) — formerly referred to as mental retardation, a term now considered outdated and stigmatizing — is a neurodevelopmental disorder characterized by significant limitations in both intellectual functioning and adaptive behavior, originating during the developmental period. Intellectual functioning refers to general cognitive abilities including reasoning, problem-solving, learning, and abstract thinking; adaptive behavior refers to the practical, social, and conceptual skills used in everyday life.
Diagnosis requires both a significantly below-average IQ (generally below 70, or approximately two standard deviations below the mean) and significant limitations in adaptive functioning — the practical, conceptual, and social skills that allow people to manage daily life independently. The DSM-5 places primary emphasis on adaptive functioning rather than IQ scores alone, recognizing that functional capacity matters more than test performance.
Intellectual disability is classified by severity:
- Mild ID (approximately 85% of cases): individuals may achieve academic skills up to a sixth-grade level with appropriate support; many live semi-independently in adulthood
- Moderate ID: significant support needs in daily living; academic progress to approximately second-grade level; usually require supervised living arrangements
- Severe ID: limited verbal communication; require substantial daily support for basic self-care activities
- Profound ID: very limited communication and self-care ability; require constant, intensive support
Causes are diverse and include genetic conditions (Down syndrome, Fragile X syndrome, Rett syndrome), prenatal exposures (alcohol, infections, toxins), perinatal complications (birth asphyxia, prematurity), and postnatal factors (severe early neglect, traumatic brain injury). For a significant proportion of cases, particularly mild ID, no specific organic cause is identified.
The most important practical takeaway: intellectual disability describes a profile of support needs, not a fixed ceiling on a person’s capacity for learning, growth, connection, or meaning. With appropriate education, therapeutic support, and community inclusion, people with intellectual disability can live rich, meaningful, and autonomous lives across a wide spectrum of ability levels.

Autism Spectrum Disorder: Social Communication and the Spectrum of Human Difference
Autism spectrum disorder (ASD) is defined by two core feature clusters: persistent differences in social communication and social interaction, and the presence of restricted, repetitive patterns of behavior, interests, or activities. It is called a spectrum because its presentations range enormously — from a minimally verbal child with significant intellectual disability and profound sensory sensitivities to a highly verbal adult with a demanding professional career who has spent decades masking autistic traits in order to fit social expectations.
The DSM-5 unified the previous separate diagnoses of autistic disorder, Asperger’s syndrome, and pervasive developmental disorder-not otherwise specified (PDD-NOS) under a single ASD umbrella in 2013. This change remains somewhat controversial — many individuals who identified strongly with their Asperger’s diagnosis feel that nuance was lost — but it reflects the empirical evidence that these presentations exist on a continuum rather than as categorically distinct conditions.
Social communication differences in ASD may include:
- Differences in the use of eye contact, facial expression, and body language — not absence of social interest, but a different social language
- Difficulty reading implicit social cues, navigating unspoken social rules, and understanding the unstated expectations that neurotypical social environments assume
- Challenges with the back-and-forth reciprocity of conversation — not because the person doesn’t want connection, but because the social code operates differently
- Differences in developing and maintaining friendships appropriate to developmental level
Restricted and repetitive behaviors may include intense, circumscribed interests pursued with unusual depth and focus; insistence on sameness and distress at unexpected changes; stereotyped movements (stimming) such as hand-flapping or rocking, which serve genuine self-regulatory functions; and sensory sensitivities — to sounds, textures, lights, tastes, or physical sensations — that can profoundly affect daily functioning and comfort.
Simon Baron-Cohen’s research on autism, including his theory of mind work and later the concept of the “extreme male brain” hypothesis, has been influential — though also debated. More recent neurodiversity frameworks, including the work of autistic scholars and advocates, emphasize that autism is a different neurotype rather than a deficit, and that many of the challenges autistic people face are as much a product of environments designed for neurotypical brains as of autism itself.
Evidence-based supports for ASD include speech-language therapy, occupational therapy, Applied Behavior Analysis (ABA — though its philosophy and ethics are actively debated within the autistic community), social skills groups, and educational accommodations. Psychological support for the anxiety, depression, and autistic burnout that often accompany ASD — particularly in those who have masked their traits extensively — is increasingly recognized as an essential component of care.

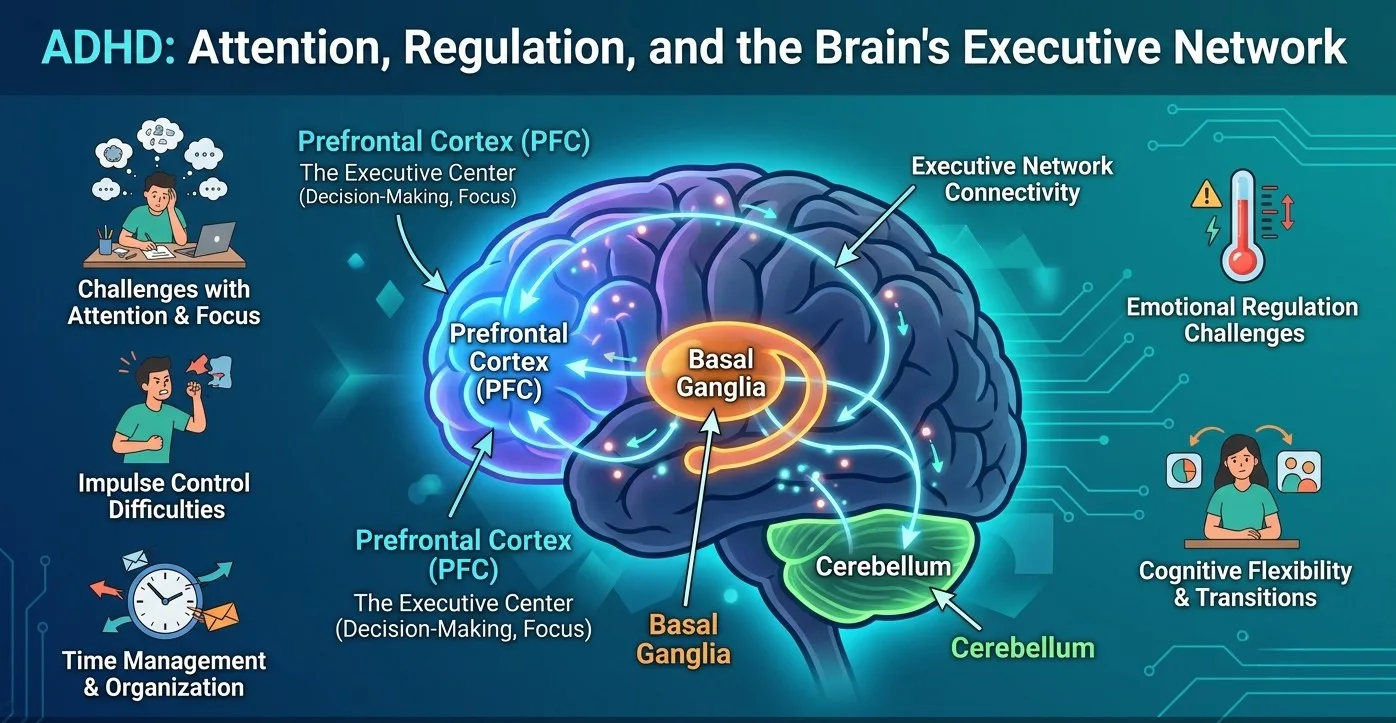
ADHD: Attention, Regulation, and the Brain’s Executive Network
Attention-deficit/hyperactivity disorder is one of the most studied and most debated neurodevelopmental disorders — and one of the most misunderstood. ADHD is not a deficit of attention so much as a dysregulation of attention: difficulty directing, sustaining, and shifting attention in ways that match situational demands, rather than an inability to pay attention to anything. Many people with ADHD can hyperfocus intensely on topics that engage them; the challenge is regulating that focus deliberately, especially in contexts of low intrinsic interest.
The DSM-5 recognizes three presentations:
- Predominantly inattentive presentation: difficulties with sustained attention, organization, follow-through, and working memory — without prominent hyperactivity or impulsivity. This presentation is more common in girls and is more frequently missed or diagnosed late
- Predominantly hyperactive-impulsive presentation: prominent motor restlessness, difficulty remaining still, excessive talking, impulsive decision-making, and difficulty waiting — without the full inattentive profile. More common in younger children
- Combined presentation: meeting criteria for both inattentive and hyperactive-impulsive symptoms — the most common presentation in clinical settings
ADHD is fundamentally a disorder of executive function — the network of cognitive processes that regulate goal-directed behavior, including working memory, cognitive flexibility, inhibitory control, planning, and emotional regulation. Russell Barkley’s influential model frames ADHD as primarily an inhibition deficit that cascades through executive function, producing downstream effects on time management, emotional regulation, motivation, and self-regulation.
The neurobiological underpinnings involve differences in the prefrontal cortex, striatum, and dopaminergic and noradrenergic neurotransmitter systems. Neuroimaging research has consistently demonstrated differences in prefrontal cortical development and function, delayed cortical maturation (typically by 2–3 years), and reduced volume in frontostriatal circuits in individuals with ADHD compared to neurotypical controls.
Effective, evidence-based approaches include stimulant medications (methylphenidate and amphetamine-based compounds), non-stimulant medications (atomoxetine, guanfacine), behavioral therapy — particularly parent training for younger children — executive function coaching, environmental accommodations (extended time, reduced distraction), and CBT for the emotional regulation and self-esteem challenges that accompany ADHD in adolescents and adults.
Specific Learning Disorders: When Intelligence and Academic Skills Diverge
Specific learning disorders (SLDs) are neurodevelopmental conditions in which a person’s academic achievement in a specific domain is significantly below what would be expected given their age, intelligence, and educational experience — and this discrepancy cannot be explained by intellectual disability, sensory impairment, or inadequate instruction. The defining feature is specificity: a circumscribed difficulty in one area (reading, writing, or mathematics) against a background of otherwise intact intellectual functioning.
The DSM-5 identifies three subtypes:
- Specific learning disorder with impairment in reading (dyslexia): the most common SLD, characterized by difficulties with accurate or fluent word recognition, poor decoding, and poor spelling. Dyslexia is a phonological processing disorder at its core — a difficulty mapping the sound units of language onto their written representations — and is neurobiological in origin, with consistent differences in left hemisphere reading network activation documented in neuroimaging research. Maryanne Wolf’s work on the reading brain and dyslexia has been particularly illuminating about what goes wrong and how structured literacy approaches can support those affected
- Specific learning disorder with impairment in written expression (dysgraphia): difficulties with spelling accuracy, grammar, punctuation, and the organization and clarity of written expression — beyond what would be expected from motor difficulties alone. People with dysgraphia often show a striking discrepancy between their verbal expressiveness and the quality of their written output
- Specific learning disorder with impairment in mathematics (dyscalculia): difficulty with number sense, arithmetic fact retrieval, calculation accuracy, and mathematical reasoning. Dyscalculia affects approximately 3–7% of children and is often underidentified compared to dyslexia, partly because mathematics difficulties are more easily attributed to poor teaching or low effort
Specific learning disorders are lifelong but highly responsive to evidence-based intervention. Structured literacy approaches — systematic, explicit, cumulative phonics instruction — represent the strongest evidence base for dyslexia. Multisensory math instruction and explicit number sense training support dyscalculia. Assistive technology (text-to-speech, dictation software, calculators) can significantly reduce the functional impact of these disorders for older students and adults.

Communication Disorders: When Language Itself Is the Challenge
Communication disorders are neurodevelopmental conditions affecting the acquisition and use of language or speech, producing significant impairment in social communication, academic achievement, or daily functioning. The DSM-5 groups them into four subtypes, each targeting a distinct aspect of communication.
Language disorder (also known as developmental language disorder or DLD) is characterized by persistent difficulties in the acquisition and use of language — including vocabulary, sentence structure, discourse, and narrative — that are not explained by hearing loss, intellectual disability, or other identified neurological condition. DLD affects approximately 7–10% of children, making it among the most prevalent neurodevelopmental conditions in existence, yet public awareness remains remarkably low. Dorothy Bishop’s advocacy for the recognition and naming of DLD has been central to raising its profile internationally.
Speech sound disorder involves persistent difficulties with the production of speech sounds — articulation errors, phonological processing errors, or both — that impair intelligibility and social communication beyond what is typical for the child’s developmental stage.
Childhood-onset fluency disorder (stuttering) is characterized by disruptions in the normal flow of speech, including repetitions of sounds, syllables, or words; prolongations of sounds; and blocks in which speech stops entirely. Approximately 5% of children stutter at some point in development; the majority recover, but around 1% persist into adulthood. The emotional and psychological dimensions — anticipatory anxiety, avoidance, and shame — are as important to address as the speech patterns themselves.
Social (pragmatic) communication disorder is a relatively new DSM-5 category describing difficulties with the social use of verbal and nonverbal communication — understanding and following the implicit rules of conversation, adjusting language to context, interpreting indirect language, and understanding what is not literally stated. It differs from ASD in the absence of restricted and repetitive behaviors; its delineation from ASD remains an area of ongoing clinical discussion.

Neurodevelopmental Motor Disorders: Movement, Coordination, and Tics
Neurodevelopmental motor disorders are a group of conditions in which the development of motor control, coordination, or movement regulation is significantly impaired. The DSM-5 includes three main categories: developmental coordination disorder, stereotypic movement disorder, and tic disorders.
Developmental coordination disorder (DCD) — also known as dyspraxia — is characterized by significant difficulty acquiring and executing coordinated motor skills, producing performance substantially below that expected for age and opportunity for skill learning. It affects approximately 5–6% of school-age children and frequently co-occurs with ADHD, DLD, and dyslexia. Children with DCD may struggle with handwriting, sports, getting dressed, using cutlery, riding a bike, and a host of other activities that require the precise sequencing and execution of motor programs. The impact on self-esteem and social participation — when a child cannot keep up with peers in physical activities — is often profound and underappreciated.
Tic disorders involve sudden, rapid, recurrent, non-rhythmic motor movements or vocalizations. The DSM-5 recognizes three subtypes:
- Tourette syndrome: the presence of both multiple motor tics and at least one vocal tic, persisting for more than one year. Tourette syndrome is often misrepresented in popular culture — the dramatic, coprolalia-involving presentation (involuntary swearing) actually represents a minority of cases. Most people with Tourette’s have a more variable, waxing-and-waning tic profile, and many develop the capacity for partial voluntary suppression over time
- Persistent (chronic) motor or vocal tic disorder: single or multiple motor or vocal tics (but not both) persisting more than one year
- Provisional tic disorder: tics present for less than one year
Stereotypic movement disorder involves repetitive, seemingly driven, non-functional motor behavior — such as hand shaking, body rocking, head banging, or self-biting — that interferes with social, academic, or other activities or results in self-injury. It is distinguished from tics by the more rhythmic, patterned quality of the movements and from ASD-related stimming by the degree of functional impairment and self-injurious potential.

Beyond the DSM-5: Other Significant Neurodevelopmental Conditions
Several important conditions are not formally classified within the DSM-5’s neurodevelopmental category but are widely recognized to have neurodevelopmental origins and profiles.
Cerebral palsy (CP) is the most common childhood physical disability, arising from damage to the developing brain before, during, or shortly after birth, producing permanent movement and posture disorders. CP is not progressive — the brain injury does not worsen — but its functional consequences evolve with growth and development. Four main types are recognized: spastic (the most common, characterized by increased muscle tone), dyskinetic (involuntary, uncontrolled movements), ataxic (affecting balance and coordination), and mixed. Cognitive and communication difficulties frequently accompany the motor presentation.
Fragile X syndrome is the most common inherited cause of intellectual disability, caused by a mutation in the FMR1 gene on the X chromosome. It produces a characteristic profile including intellectual disability of variable severity, social anxiety, ADHD features, sensory sensitivities, and often features overlapping with autism spectrum disorder.
Fetal alcohol spectrum disorders (FASDs) arise from prenatal alcohol exposure and produce a range of physical, cognitive, behavioral, and social-emotional difficulties. They represent a significant and largely preventable category of neurodevelopmental impairment.
Schizophrenia, though classified separately in the DSM-5 as a psychotic disorder, is increasingly understood to have important neurodevelopmental dimensions — with evidence of subtle cognitive and social difficulties predating psychotic onset by years, and neurobiological models emphasizing disrupted neurodevelopment of prefrontal and temporal cortical networks.
Causes and Risk Factors Across Neurodevelopmental Disorders
Neurodevelopmental disorders do not have single, simple causes. They arise from the complex interaction of multiple genetic, epigenetic, and environmental factors that influence brain development across the prenatal period, birth, and early childhood.
Genetic factors play a substantial role across virtually all neurodevelopmental disorders. Twin studies consistently demonstrate high heritability for ADHD, ASD, dyslexia, and intellectual disability. However, the genetics are complex: most neurodevelopmental disorders are polygenic (influenced by many genes of small effect) rather than monogenic, and identified genetic variants account for only a proportion of observed risk. Rare copy number variants (CNVs) — deletions or duplications of chromosomal segments — contribute to ASD, intellectual disability, and schizophrenia risk.
Environmental risk factors include:
- Prenatal exposures: maternal infections, alcohol (FASDs), certain medications, environmental toxins (lead, mercury, pesticides), and extreme maternal stress during pregnancy
- Perinatal factors: premature birth and low birth weight, birth asphyxia, neonatal infections, and hyperbilirubinemia
- Postnatal factors: severe early deprivation (as in the famous Romanian orphanage studies), traumatic brain injury, and early childhood infections affecting the central nervous system
- Advanced parental age: particularly paternal age, associated with increased rates of de novo genetic mutations linked to ASD and intellectual disability
An important reframe: the causes of neurodevelopmental disorders are not moral failures. They are biological processes. Seeking information, accessing diagnosis, and pursuing support are not responses to failure — they are responses to real neurological differences that deserve understanding and accommodation.

The Neurodiversity Paradigm: Reframing Difference
The concept of neurodiversity — coined by sociologist Judy Singer in the late 1990s — offers a framework that complements, rather than replaces, the medical understanding of neurodevelopmental disorders. Neurodiversity holds that neurological variation is a natural and valuable form of human diversity, and that conditions like autism, ADHD, dyslexia, and DLD represent different cognitive styles rather than simply deficits.
This framework does not deny that neurodevelopmental conditions can produce genuine functional challenges — sometimes severe ones. It does insist that many of those challenges are amplified by environments, educational systems, and social structures designed exclusively for neurotypical brains, and that with appropriate accommodation and support, neurodivergent people can and do flourish.
The neurodiversity paradigm has shifted how many clinicians, educators, and researchers approach assessment and intervention — from a purely deficit-reduction model toward one that also identifies and builds on strengths, advocates for accommodations rather than normalization, and centers the lived experience and preferences of the neurodivergent person in planning their support.
FAQs about Neurodevelopmental Disorders
What is the most common neurodevelopmental disorder?
ADHD and developmental language disorder (DLD) compete for the title of most prevalent neurodevelopmental condition, depending on the population and diagnostic criteria used. ADHD affects approximately 5–7% of children globally and persists into adulthood for the majority. DLD affects approximately 7–10% of children, making it more prevalent than autism spectrum disorder by a wide margin — yet far less recognized by the general public. Dyslexia, with prevalence estimates of 5–17% depending on criteria, is the most common specific learning disorder. Across all categories, neurodevelopmental conditions collectively affect between 10% and 15% of children, representing an enormous proportion of any school-age population.
Can neurodevelopmental disorders be cured?
Neurodevelopmental disorders cannot be “cured” in the traditional sense — they reflect fundamental differences in how the brain is organized and functions, not illnesses to be eliminated. What does change substantially is functional capacity and quality of life. Early, intensive, evidence-based intervention — tailored to the specific disorder and the individual’s profile — can produce meaningful and often dramatic improvements in communication, learning, self-regulation, and adaptive functioning. Many adults with ADHD, dyslexia, or high-support-needs autism lead fully satisfying, productive lives with appropriate accommodations, strategies, and support. The goal of intervention is not to make a neurodivergent person neurotypical but to reduce functional barriers and build genuine capacity for the life they want.
How are neurodevelopmental disorders diagnosed?
Diagnosis involves a comprehensive, multidisciplinary evaluation that includes clinical interview, developmental history, behavioral observation, and standardized psychometric testing across relevant domains. Depending on the condition, assessment may be conducted by a developmental pediatrician, child psychiatrist, clinical psychologist, neuropsychologist, speech-language pathologist, or a multidisciplinary team combining several specialists. There are no biomarkers, blood tests, or brain scans that diagnose neurodevelopmental disorders — diagnosis is based on behavioral and functional criteria. Assessment should always include evaluation of adaptive functioning, not just test scores, and should gather information from multiple informants (parents, teachers, the individual) across multiple settings. Differential diagnosis — ruling out other conditions that may explain the presentation — is an essential component of the evaluation process.
Do neurodevelopmental disorders occur together?
Yes — and more often than not. Co-occurrence of multiple neurodevelopmental conditions in the same individual is the rule rather than the exception. ADHD and dyslexia co-occur in approximately 25–40% of cases. Autism and ADHD co-occur in a substantial proportion of autistic individuals. Developmental language disorder frequently co-occurs with dyslexia, ADHD, and developmental coordination disorder. Intellectual disability commonly accompanies autism spectrum disorder. This pattern of overlap — sometimes called comorbidity, though the term implies separability that may not exist — reflects shared genetic and neurobiological risk factors across conditions. For anyone receiving a diagnosis of a neurodevelopmental disorder, comprehensive assessment across related domains is important to ensure that co-occurring conditions are identified and addressed rather than missed.
When should a parent seek an evaluation for a possible neurodevelopmental disorder?
The right time is whenever a parent has a concern — there is no benefit to waiting. Early identification consistently leads to better outcomes across all neurodevelopmental conditions because intervention during the period of peak neuroplasticity is more effective. Specific signs that warrant prompt evaluation include: significant language delay or loss of previously acquired language skills at any age; persistent behavioral difficulties that do not respond to consistent parenting approaches; significant academic struggles despite adequate instruction and effort; marked differences in social interaction, communication, or play compared to same-age peers; motor difficulties affecting daily activities disproportionate to age; or any regression in developmental milestones. Pediatricians, developmental specialists, school psychologists, and speech-language pathologists are all appropriate starting points for referral depending on the specific area of concern.
Do neurodevelopmental disorders affect adults too?
Absolutely — and the recognition of neurodevelopmental disorders in adults is an area of significant growth in clinical practice. Most neurodevelopmental conditions are lifelong, and many adults received no diagnosis in childhood — either because the condition was mild enough to compensate for in early school years, because assessment was unavailable, because the presentation was atypical (as is common for women with ADHD or autism), or because less was known about the condition at the time. Adult diagnoses of ADHD, autism, dyslexia, and DLD are increasingly common and can be profoundly validating — providing explanatory frameworks for lifelong experiences of difference that may previously have been attributed to character flaws, lack of effort, or social inadequacy. Adult diagnosis opens the door to appropriate accommodations, evidence-based treatment, and community belonging.
Is there a link between neurodevelopmental disorders and mental health?
The link is strong, consistent, and clinically important. People with neurodevelopmental disorders experience significantly elevated rates of anxiety, depression, low self-esteem, and other mental health difficulties compared to the general population. These mental health challenges are not intrinsic to the neurodevelopmental condition itself — they are frequently the accumulated consequence of years of struggling in environments not designed for the person’s neurotype: repeated academic failure, social rejection or misunderstanding, years of being told you are lazy or not trying hard enough, and the exhaustion of masking or compensating for differences that were never understood or accommodated. Addressing the mental health dimensions of neurodevelopmental disorders is not secondary to treating the primary condition — it is an integral part of comprehensive, person-centered care.
Bibliography
- American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.). APA Publishing.
- Barkley, R. A. (2015). Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment (4th ed.). Guilford Press.
- Bishop, D. V. M. (2014). Ten questions about terminology for children with unexplained language problems. International Journal of Language and Communication Disorders, 49(4), 381–415.
- Baron-Cohen, S. (2002). The extreme male brain theory of autism. Trends in Cognitive Sciences, 6(6), 248–254.
- Wolf, M. (2007). Proust and the Squid: The Story and Science of the Reading Brain. HarperCollins.
- Singer, J. (1999). Neurodiversity: The Birth of an Idea. Self-published.
- Gillberg, C. (2010). The ESSENCE in child psychiatry: Early symptomatic syndromes eliciting neurodevelopmental clinical examinations. Research in Developmental Disabilities, 31(6), 1543–1551.
- Thapar, A., Cooper, M., & Rutter, M. (2017). Neurodevelopmental disorders. The Lancet Psychiatry, 4(4), 339–346.
Use this citation format to reference the article clearly and help readers find the original source.
PsychologyFor. (2026). The 7 Types of Neurodevelopmental Disorders (Symptoms and Causes). PsychologyFor. https://psychologyfor.com/the-7-types-of-neurodevelopmental-disorders-symptoms-and-causes/