Tricipital Reflex: What It Is, Physiology, And How It Is Analyzed
The neurological examination is, together with the anamnesis, the basis for the diagnosis of pathologies of the nervous system. Although many complex tests can be performed to evaluate muscle tone and the intensity of contractions, one of the first steps when suspecting a problem at the nervous system level is always to quantify deep tendon reflexes
These reflexes are fast and involuntary, since they do not pass through the brain and are processed at the level of the spinal cord. Due to their variety and knowledge about them, it can be detected very accurately if any type of damage has occurred in the spinal cord and, if so, it is also possible to locate the injury very precisely. When deep tendon reflexes are quantified, the strength and speed of the contraction are measured, as well as the symmetry (or lack thereof) of the response and the homogeneity of reaction between different parts of the body.
In this type of test, it is not so important to put a number on each reflex from 1 to 5, but it is important to quantify the variability between the different sections and neuronal routes in the patient. Based on these very interesting premises, we tell you everything about the triceps reflex
The triceps reflex is a type of deep tendon reflex, so before looking at it, we must lay some foundations in terms of medical terminology.
The deep tendon reflexes are a type of spinal reflex, whose route of action is extremely circumscribed and very fast These types of actions do not pass directly through the brain, hence the speed of the association between the stimulus and the response.
When a force is applied to the critical point of the muscular environment, it lengthens involuntarily. Then, the neuromuscular spindle (sensory receptors within the muscle) send the mechanical stress signal to an afferent neuron, which in turn contacts the nervous center. The dorsal root ganglia collect this stimulus, which is interpreted directly in the gray matter of the spinal cord. Finally, the axons of the motor neuron leave the spinal cord and send the muscle contraction signal.
As you can see, we are faced with a very circumscribed closed circuit: spindle-afferent neuron-spinal cord-motor neuron. Because the information does not pass through the brain and is always interpreted at the same level, it is possible to detect neurological failures very accurately by quantifying deep tendon reflexes. The most important are the following:
What is the triceps reflex?
As we have said, the triceps reflex is a type of osteotendinous reflex, and at the same time myotatic, since the synaptic connection is made at the level of the spinal cord (and not the brain). To evaluate its functionality, a force is applied to the triceps tendon, located above the elbow (in the olecranon) With this reflex, the C6, C7 (predominant) and C8 nerve roots come into play, or in other words, the integrity of the musculocutaneous nerve.
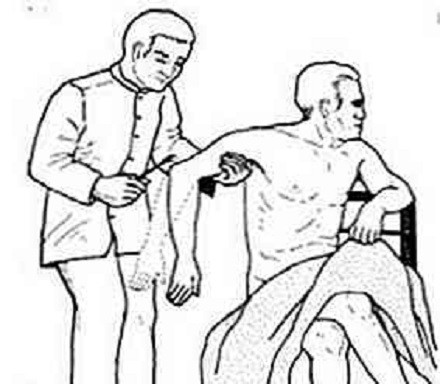
To perform this test, support the patient’s forearm (ideally placing it on the thigh), with the arm in a position halfway between flexion and extension. Once the desired position has been reached, the triceps tendon must be located and struck at its base of insertion.
When this sudden force is applied, the forearm is expected to extend rapidly If the absence of movement is absolute (areflexia), myopathy, neuropathy, spondylosis and other clinical entities of a neuromuscular nature are suspected.
How is it analyzed in patients?
In order to homogenize a test as subjective as this, the National Institute of Neurological Disorders and Stroke devised a numerical scale applicable in all cases. Once percussion occurs on the tendon of interest, the response is quantified based on the following parameters:
Depending on the rest of the answers, A triceps reflex between 2 and 3 can be considered “normal,” as long as it occurs in the same way on both body planes (left and right arm). A value of 0 is conceived as areflexia, while a value of 4-5 is hyperreflexia.
Additionally, it should be noted that each of these values can be further circumscribed with a (+) or a (-), reflecting that the patient’s condition is between two of the figures. As you can imagine, a 3+ and a 4- can be the same for two different evaluators, so we repeat that the sign and the number are not as important as the homogeneity between results within the same patient.
Interpretation of the results
An areflexia may show damage to a particular nerve pathway or, failing that, an abnormality in the spine or the entire nervous system and general condition of the patient. Without going any further, some of the deep tendon reflexes are better predictors of neuropathy derived from diabetes than many other tests and subjective symptoms of the patient.
For its part, hyperreflexia may indicate damage to the upper motor neurons, while hyporeflexia or areflexia usually indicate lesions in the lower motor neurons. In general, a range of 1+ to 3+ is estimated to be within normality if the response is symmetrical. Anyway, Even an absent reflex can be considered normal in some patients if this is not accompanied by other symptoms and conditions that allow us to assume a neurological problem.
Today, peripheral neuropathies are the most common cause of absence of reflexes in general society. The triggers for this condition are very varied: diabetes, alcoholism, amyloidosis, uremia, vitamin deficiencies, pernicious anemia, remote cancer, presence of toxins in the body and many other etiological agents. Once an abnormality is detected in the triceps reflex (or any osteotendinous reflex), it is necessary to undergo more tests until the patient’s problem is found.
Summary and final notes
As you may have seen, the triceps reflex (and deep tendon reflexes in general) is essential for clinical semiology, especially when detecting neuropathy of the peripheral nervous system. These reflexes are very important in the medical field, because by not “passing” through the brain, the damage can be clearly detected in a very specific environment to the involved section of the spinal cord.
Thus, reflexes are very useful when detecting pathologies, but they must be accompanied by a series of accessory tests to confirm or rule out a diagnosis. Deep tendon reflexes are the first step in suspecting a disease, but they never make up the complete diagnosis on their own.


")





