A patient sits across from a neuropsychologist, nervous about what the assessment will reveal. The clinician places a card on the table showing geometric shapes—a large circle, a diamond, a small square positioned to the side. Ten seconds pass. The card is removed. “Draw what you saw,” the psychologist instructs, sliding a blank sheet of paper forward. The patient’s hand hovers uncertainly over the page, struggling to recall the exact configuration of shapes that seemed so clear moments ago. This simple task—viewing designs briefly and reproducing them from memory—forms the core of the Benton Visual Retention Test, one of neuropsychology’s most enduring and valuable assessment tools for evaluating how the brain processes, stores, and retrieves visual information.
Developed by neuropsychologist Arthur Benton, this test has been used for decades to assess visual memory, visual perception, and visuoconstructive abilities in people ranging from children as young as eight to elderly adults approaching ninety. Unlike tests measuring verbal memory or abstract reasoning, the Benton focuses specifically on the brain’s capacity to work with visual and spatial information—the kind of processing that lets you remember where you parked your car, recognize faces, navigate familiar routes, or copy a drawing accurately. When these abilities are impaired through brain injury, stroke, dementia, or neurological disease, the consequences affect daily functioning in profound ways. You get lost in familiar places. You can’t remember what someone looks like. You struggle to perform tasks requiring spatial awareness like parallel parking or organizing objects. The Benton Visual Retention Test helps clinicians identify and quantify these impairments, providing crucial information for diagnosis, treatment planning, and tracking disease progression. What makes this test particularly valuable is its sensitivity to subtle cognitive deficits that might not be apparent in casual observation but significantly impact functioning. A person might seem cognitively intact in conversation yet show clear impairment when asked to reproduce simple geometric designs. The test reveals problems with attention, visual processing, spatial relationships, and memory that other assessments might miss. This article explores the characteristics that make the Benton Visual Retention Test a foundational neuropsychological instrument, the specific methods for administering and scoring it, the cognitive abilities it measures, and how clinicians interpret results to understand brain function and identify pathology.
What the Benton Visual Retention Test Measures
The Benton Visual Retention Test assesses multiple cognitive domains simultaneously, making it a rich source of information about brain function. At its core, the test evaluates visual memory—the capacity to encode, store, and retrieve visual information. When you view a design for ten seconds and then reproduce it from memory, you’re demonstrating your brain’s ability to form and maintain a mental representation of spatial information.
But visual memory isn’t a single process. It involves multiple brain systems working together. First, you must accurately perceive the design—seeing the shapes, their sizes, their spatial relationships. This requires intact visual perception, the ability to make sense of incoming visual information. Problems with visual perception might manifest as not seeing parts of the design, misidentifying shapes, or failing to notice spatial relationships between elements.
Once perceived, the design must be encoded into memory, a process requiring attention and working memory. You’re holding the visual information actively in mind, maintaining it across the brief interval before reproduction. Deficits in attention or working memory impair this process, causing designs to fade or become distorted in memory before you can draw them.
Reproduction requires visuoconstructive abilities—translating the mental representation back into a physical drawing. This involves visual-motor integration, spatial planning, and motor execution. You must plan how to draw each shape, where to place it relative to others, and execute those movements accurately. Problems with visuoconstructive abilities might result in correctly remembering what you saw but struggling to reproduce it accurately on paper.
The test also reveals information about hemispatial neglect—the tendency to ignore one side of space, typically resulting from right hemisphere brain damage. If someone consistently omits figures on the left side of designs or places all figures toward the right side of the page, this suggests spatial attention deficits characteristic of neglect.
Additionally, the test provides information about executive functions including planning, organization, and cognitive flexibility. Successfully reproducing complex designs requires planning the sequence of drawing, organizing spatial relationships, and flexibly adjusting when mistakes occur. Impairments in these areas produce characteristic error patterns.
Test Structure and Design
The Benton Visual Retention Test consists of three equivalent alternate forms—typically labeled C, D, and E—each containing ten designs. These alternate forms allow for repeated testing while minimizing practice effects. If you’re assessing someone multiple times to track recovery from brain injury or progression of dementia, you can use different forms to prevent them from simply remembering the specific designs from previous administrations.
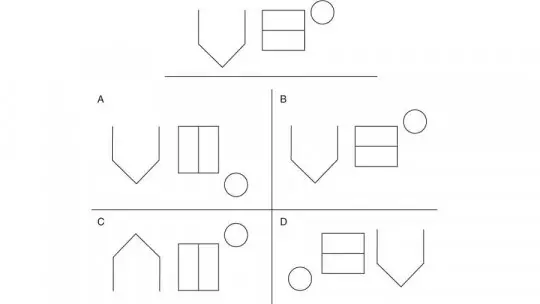
Each of the ten designs in a form presents geometric figures arranged on a card measuring approximately 8.5 by 5.5 inches. The first two designs contain a single major geometric figure—perhaps a large circle or diamond. The remaining eight designs increase in complexity, each containing two major geometric figures plus a smaller peripheral figure positioned to the left or right. This design structure allows assessment of both simple and more complex visual memory demands.
The geometric figures include basic shapes—circles, squares, diamonds, triangles—as well as more complex forms. They vary in size, with clear distinctions between major figures and smaller peripheral elements. The spatial relationships between figures are critical—how far apart they’re positioned, whether they’re aligned vertically or horizontally, whether the small figure is left or right of the major figures. These spatial details are what make the test challenging and what reveal subtle cognitive impairments.
The test materials include the stimulus cards showing the designs, a response booklet containing blank pages where the examinee draws their reproductions, and a detailed manual providing administration instructions, scoring criteria, and normative data for different age groups and education levels. The simplicity of materials—just cards and paper—makes the test portable and easy to administer in various settings.
Administration Methods: Five Different Approaches
One of the Benton Visual Retention Test’s strengths is its flexibility in administration. Five different methods are available, each assessing slightly different aspects of visual processing and memory. Clinicians select the method most appropriate for the clinical question they’re addressing and the patient’s capabilities.
Administration A: Standard Memory Task
This is the most commonly used method. The examiner shows each design for ten seconds, then removes it. The examinee must reproduce the design from memory on a blank page. This ten-second exposure followed by immediate reproduction assesses immediate visual memory—the ability to encode and briefly retain visual-spatial information. This method provides the standard normative data most clinicians reference when interpreting performance.
Administration B: Reduced Exposure Time
This method is identical to Administration A except the exposure time is reduced to five seconds. The shorter viewing time increases task difficulty, requiring more efficient encoding and potentially revealing more subtle memory deficits. Some patients perform adequately with ten-second exposure but struggle with five seconds, suggesting borderline memory capacity that breaks down under increased demand.
Administration C: Copy Task
In this method, the design remains visible while the examinee copies it. There’s no time limit—they can take as long as needed to reproduce the design while looking at it. This method eliminates the memory component, assessing only visual perception and visuoconstructive abilities. If someone performs poorly on Administration A but normally on Administration C, this suggests the problem is memory rather than perception or construction. Conversely, poor performance even when copying indicates perceptual or constructional deficits.
Administration D: Delayed Reproduction
This method shows each design for ten seconds, but then imposes a fifteen-second unfilled delay before reproduction begins. During this delay, the examinee isn’t allowed to rehearse or draw—they simply wait. The delay increases memory demands, as the visual information must be maintained across a longer interval. This method can reveal memory problems that aren’t apparent with immediate reproduction and provides information about how quickly visual memories decay.
Administration M: Multiple Choice Recognition
In this variant, available in Forms F and G, the examinee views the design for ten seconds, then chooses the correct design from four multiple-choice options. This recognition format eliminates the need to draw, removing visuoconstructive demands and motor requirements. It’s particularly useful for patients with motor impairments, severe tremor, or visual-motor problems that would confound standard administration. The multiple-choice format assesses visual memory through recognition rather than recall, generally an easier task that can help determine whether memory problems are related to retrieval difficulties or encoding/storage failures.
Scoring Systems: Quantitative and Qualitative Analysis
The Benton Visual Retention Test employs two complementary scoring systems that provide both quantitative measures of overall performance and qualitative information about specific types of errors. This dual approach offers rich diagnostic information beyond a simple total score.
The Correct Score
The correct score uses an all-or-none system for each of the ten designs. A design receives one point if reproduced correctly according to specified criteria, or zero points if any error is present. The total correct score ranges from zero to ten. This scoring is strict—even a single minor error results in zero points for that design. The stringent criteria ensure the test is sensitive to subtle impairments.
Correct reproductions must meet specific standards: all figures must be present, shapes must be recognizable and reasonably accurate, spatial relationships must be preserved, sizes must be appropriate, and no additional elements can be added. The manual provides detailed criteria and examples of designs that do and don’t meet standards for correctness.
The correct score is compared to normative data adjusted for age, education level, and sometimes IQ. These norms allow clinicians to determine whether performance is within expected range or indicates impairment. For example, a sixty-year-old with twelve years of education might be expected to score eight or nine, while a score of four or five would indicate significant impairment.
The Error Score
While the correct score provides an overall performance measure, the error score offers detailed qualitative analysis. This system identifies and categorizes specific types of errors, providing information about the nature of cognitive impairment. The error score can range from zero to twenty-six, as some designs can produce multiple errors.
Six major error categories are identified, each revealing different cognitive problems. Omissions occur when figures are left out entirely. This might indicate memory failure, attentional problems, or hemispatial neglect if omissions are consistently on one side. A patient who forgets to include the small peripheral figure shows different impairment than one who omits major central figures.
Distortions involve changes to figure shapes. The circle becomes egg-shaped, the diamond looks like a trapezoid, angles aren’t preserved. Distortions suggest visuoperceptual problems or visuoconstructive difficulties—the person saw or remembered the shape inaccurately, or couldn’t translate their mental image into an accurate drawing.
Perseverations are repetitions or continuations of figures or elements that shouldn’t be repeated. The patient might draw the same figure twice, add extra components, or continue a pattern beyond what the design showed. Perseveration typically indicates frontal lobe dysfunction affecting cognitive flexibility and inhibition.
Rotations involve turning figures more than forty-five degrees from their correct orientation. The diamond appears as a square, vertical alignments become horizontal. Rotations can indicate spatial processing deficits or problems with spatial orientation, often associated with parietal lobe dysfunction.
Misplacements occur when figures are positioned incorrectly relative to each other. The small peripheral figure that should be on the left appears on the right, or figures that should be separated are drawn overlapping. Misplacements reveal problems with spatial relationships and visual-spatial memory.
Size errors involve figures drawn significantly too large or too small relative to other elements. The major figures might be tiny while the peripheral figure is huge, or everything is miniaturized or enlarged. Size errors can indicate problems with visual perception, spatial scaling, or sometimes psychiatric conditions.
Clinical Applications and What Results Reveal
The Benton Visual Retention Test serves multiple clinical purposes, each leveraging its sensitivity to different types of brain dysfunction. Its primary use is identifying and characterizing acquired neurological deficits—brain damage from injuries, strokes, tumors, or disease. When someone suffers traumatic brain injury, the test helps determine whether visual memory and spatial processing were affected and to what degree.
The test is particularly sensitive to dementia and Alzheimer’s disease. Visual memory often deteriorates earlier than verbal memory in Alzheimer’s, and the Benton can identify these deficits before they’re apparent in daily life. Research shows that poor performance on the test, particularly on the copy version, predicts increased risk for developing Alzheimer’s disease. The test helps distinguish between normal age-related memory changes and pathological decline requiring intervention.
For stroke patients, the test reveals the functional consequences of brain damage. Right hemisphere strokes affecting parietal regions often produce hemispatial neglect visible in Benton performance—consistent omission of figures on the left, crowding of all reproductions toward the right side of the page. Left hemisphere strokes might produce different error patterns depending on location and extent of damage.
The test identifies learning disabilities in children, particularly those involving visual-spatial processing. A child who performs well on verbal memory tests but poorly on the Benton shows a specific profile suggesting nonverbal learning disability. This information guides educational interventions and helps explain academic difficulties that seem inconsistent with overall intelligence.
Industrial and environmental medicine uses the test to assess neurotoxic effects of chemical exposures. The test is included in batteries evaluating workers exposed to lead, mercury, pesticides, or other neurotoxins. Performance declines can indicate subclinical neurotoxicity before other symptoms become apparent, allowing intervention before significant permanent damage occurs.
Psychiatric applications include differentiating depression-related cognitive impairment from dementia. Both conditions can impair memory, but error patterns differ. Depressed patients might show poor effort or inconsistent performance, while dementia patients show characteristic error types. The test also helps identify cognitive deficits in schizophrenia, particularly problems with spatial processing and organization.
Interpreting Performance: What Scores Mean
Interpreting Benton Visual Retention Test results requires considering multiple factors beyond the raw scores. Age significantly affects performance—older adults typically score lower than younger adults due to normal age-related declines in processing speed and working memory. The normative data accounts for this by providing age-adjusted expectations.
Education level also influences performance. More educated individuals typically score higher, possibly reflecting better developed cognitive strategies, greater comfort with test-taking, or neurological protection from cognitive reserve. Someone with eight years of education scoring six might be performing normally for their demographic, while someone with a graduate degree scoring six shows impairment.
The pattern of errors matters as much as the total score. A patient scoring five with mostly omission errors shows different impairment than one scoring five with mostly rotation and misplacement errors. The first suggests memory or attention problems, the second indicates spatial processing deficits. A neuropsychologist examines which specific errors occurred and on which designs to form hypotheses about underlying brain dysfunction.
Comparing performance across administration methods provides diagnostic information. If someone performs poorly on Administration A (ten-second memory) but normally on Administration C (copying), the problem is clearly memory rather than perception or construction. If they perform poorly on both, the deficit lies in perception or constructional abilities rather than memory specifically.
Discrepancies between the correct score and error score can be revealing. Someone might have a low correct score but relatively few errors if the errors that occurred violated the strict correct score criteria. Conversely, high error scores with moderate correct scores suggest multiple types of problems affecting performance.
Advantages and Limitations
The Benton Visual Retention Test offers several advantages that explain its enduring popularity. Administration is quick—typically five to ten minutes—making it practical even in busy clinical settings. The simple materials and straightforward procedures allow reliable administration by trained technicians. The availability of alternate forms permits repeated testing without practice effects, crucial for tracking recovery or decline over time.
The test’s sensitivity to subtle deficits makes it valuable for early detection of neurological problems. Someone might perform normally on gross neurological examination yet show clear impairment on the Benton, revealing problems requiring further investigation. The detailed error analysis provides qualitative information that guides diagnosis beyond what total scores alone reveal.
Extensive normative data spanning ages eight to eighty-nine and accounting for education levels make interpretation straightforward. The test has been used for decades in thousands of studies, providing robust evidence for its validity and clinical utility across diverse populations and conditions.
However, limitations exist. The test assesses immediate memory only—there’s no delayed recall component to evaluate how information is retained over longer intervals. Performance can be affected by motor problems, tremor, or arthritis that impair drawing ability even when cognition is intact. The multiple-choice version addresses this limitation but measures different processes than standard administration.
Cultural and educational factors can influence performance in ways the norms don’t fully capture. Someone unfamiliar with geometric shapes or uncomfortable with testing situations might perform poorly despite intact cognition. The test also requires cooperation and effort—someone intentionally performing poorly or not trying their best can produce misleadingly low scores.
The test measures only one aspect of memory—visual-spatial memory—and doesn’t assess verbal memory, recognition memory, or other cognitive domains. A comprehensive neuropsychological evaluation requires additional tests. The Benton provides valuable information but isn’t sufficient alone for complete cognitive assessment.
FAQs About the Benton Visual Retention Test
What exactly does the Benton Visual Retention Test measure?
The test measures multiple related cognitive abilities including visual memory, visual perception, and visuoconstructive skills. Visual memory is the capacity to encode, store, and retrieve visual information—in this case, remembering geometric designs after brief exposure. Visual perception refers to accurately processing incoming visual information, seeing shapes, sizes, and spatial relationships correctly. Visuoconstructive abilities involve translating mental images into physical drawings through visual-motor integration and spatial planning. The test also reveals attention problems, spatial neglect, and executive function issues. Because reproducing designs from memory requires all these abilities working together, the test provides rich information about how the brain processes visual-spatial information. Poor performance could reflect problems with any of these components, which is why clinicians analyze specific error patterns to determine the nature of impairment.
How is the test administered and how long does it take?
Administration typically takes five to ten minutes. The examiner shows the patient ten cards, each containing geometric designs. In the standard method, each design is shown for ten seconds, then removed, and the patient draws what they remember on blank paper. There are five administration methods available: ten-second viewing with immediate reproduction, five-second viewing with immediate reproduction, copying while viewing the design, ten-second viewing with fifteen-second delay before reproduction, and multiple-choice recognition format. The examiner selects the method appropriate for the clinical question and patient’s abilities. The test is individually administered in a quiet setting with minimal distractions. Materials needed include the stimulus cards, response booklet with blank pages, and pencils. The simplicity and brief duration make it practical even for patients with limited attention or stamina.
What ages can take the Benton Visual Retention Test?
The test is appropriate for individuals aged eight years to elderly adulthood, with normative data available for ages eight to eighty-nine. For children aged eight to fourteen, special pediatric norms are used that account for developmental differences in visual-spatial abilities and motor skills. Adult norms apply from age fifteen onward, with adjustments for age groups throughout adulthood and into old age since visual memory naturally declines somewhat with aging. Education level is also considered when interpreting scores, as more education correlates with better performance. The test’s broad age range makes it useful across the lifespan, from identifying learning disabilities in children to detecting dementia in elderly adults. However, children under eight typically lack the motor control and cognitive maturity needed for reliable administration.
How are results scored and interpreted?
Two scoring systems are used. The correct score gives one point for each design reproduced without errors, ranging from zero to ten. This provides an overall performance measure compared to age and education-adjusted norms. The error score identifies and counts specific error types including omissions, distortions, perseverations, rotations, misplacements, and size errors, ranging from zero to twenty-six. Higher error scores indicate more severe impairment. Clinicians interpret results by comparing scores to normative data and analyzing error patterns. For example, consistent omissions on one side suggest hemispatial neglect, while numerous rotations indicate spatial processing problems. Performance is also compared across different administration methods—poor memory performance but normal copying suggests memory deficits rather than perceptual or constructional problems. The pattern and types of errors provide diagnostic information about underlying brain dysfunction.
What conditions does the test help diagnose?
The test is sensitive to various neurological and neuropsychological conditions. It helps identify traumatic brain injury effects, particularly damage affecting visual memory and spatial processing. It’s highly sensitive to dementia including Alzheimer’s disease, often detecting impairment before other symptoms are obvious. Stroke patients show characteristic patterns—right hemisphere strokes often produce left-sided neglect visible in test performance. The test identifies learning disabilities in children, particularly nonverbal learning disabilities affecting spatial reasoning. It’s used in industrial medicine to detect neurotoxic effects from chemical exposures including lead, mercury, and pesticides. The test also helps differentiate depression-related cognitive impairment from dementia and identifies spatial processing deficits in schizophrenia. However, the test alone doesn’t diagnose conditions—it provides data contributing to comprehensive neuropsychological evaluation.
Can the test be given multiple times to the same person?
Yes, the test is specifically designed for repeated administration through three equivalent alternate forms. Using different forms minimizes practice effects—the patient isn’t simply remembering the specific designs from previous testing. Repeated testing is valuable for tracking recovery after brain injury, monitoring dementia progression, assessing treatment effects, or evaluating whether neurotoxic exposures have worsened cognitive function over time. The interval between administrations depends on the clinical purpose—days or weeks when monitoring acute recovery, months or years when tracking chronic conditions. However, some practice effect can occur even with alternate forms, particularly regarding general test-taking strategies and comfort with the task. Clinicians account for this when interpreting serial results. The availability of multiple equivalent forms is a significant advantage over tests that can only be given once without practice confounding results.
What do different error types indicate about brain function?
Each error category suggests different cognitive problems. Omissions indicate memory failure, attention deficits, or when consistently on one side, hemispatial neglect from right hemisphere damage. Distortions suggest visuoperceptual problems or visuoconstructive difficulties—problems accurately seeing or drawing shapes. Perseverations indicate frontal lobe dysfunction affecting cognitive flexibility and inhibition—the person can’t stop a response that should end. Rotations suggest spatial processing deficits or problems with spatial orientation, often associated with parietal lobe dysfunction. Misplacements reveal problems with spatial relationships and visual-spatial memory, indicating difficulty maintaining accurate mental representations of how elements relate spatially. Size errors can indicate perceptual problems, spatial scaling difficulties, or sometimes psychiatric conditions. Analyzing which error types predominate and on which designs helps neuropsychologists form hypotheses about which brain regions or systems are impaired.
How does the test compare to other memory assessments?
The Benton Visual Retention Test specifically assesses visual-spatial memory, distinguishing it from tests measuring verbal memory like word lists or story recall. Its focus on immediate reproduction from memory differs from tests assessing delayed recall or recognition memory. The brief administration time makes it more practical than lengthy comprehensive memory batteries. The multiple administration methods provide flexibility that many memory tests lack. Compared to other visual memory tests, the Benton’s geometric designs eliminate verbal mediation strategies—you can’t easily verbally describe the designs to remember them, ensuring assessment of true visual memory. The extensive normative data and decades of research supporting its validity give it advantages over newer instruments. However, its limitation to immediate memory means it doesn’t assess long-term retention like tests with delayed recall components. The Benton is typically used as part of comprehensive neuropsychological batteries alongside tests assessing other cognitive domains rather than as a standalone measure.
By citing this article, you acknowledge the original source and allow readers to access the full content.
PsychologyFor. (2025). Benton Visual Retention Test: Characteristics and Method of Use. https://psychologyfor.com/benton-visual-retention-test-characteristics-and-method-of-use/