Open a neuroscience textbook and you’ll encounter a curious character stretched across the brain’s surface: a lopsided “little man” with enormous lips and hands, tiny legs tucked along a narrow ridge of cortex. That figure is the homunculus—Latin for “little man”—and it represents one of the most enduring insights in brain science. Created from the pioneering work of neurosurgeon Wilder Penfield, the sensory and motor homunculi are visual maps that show how the brain organizes feeling and movement for every part of the body. The shape looks comical at first, but the message is serious: the brain devotes far more neural real estate to parts of the body that require fine sensation and precise control—especially the hands, lips, and tongue—than to areas that need only broad, coarse signals. Understanding why this is true, how the maps were drawn, and where they live in the brain gives a powerful, practical way to think about everything from stroke symptoms and surgical planning to skill building, rehabilitation, and even the future of neurotechnology.
As a psychologist, this guide aims to make the science intuitive and genuinely useful. We’ll walk through what the homunculus is and isn’t, where the sensory and motor strips are located, how Penfield mapped them in awake brain surgery, and why the figure looks so distorted. You’ll also see how the maps explain real-life experiences like fingertip dexterity and speech, how they guide clinicians at the bedside and in the operating room, and how they remain central to cutting-edge work in brain–computer interfaces. Along the way, we’ll disentangle myths from modern updates and show simple ways to “feel” your own homunculus in action. If you’ve ever wondered why the fingertips feel exquisitely detailed while the middle of the back feels vague, or why a small injury to the mouth can disrupt speech more than you might expect, the homunculus provides a clear, memorable answer.
A plain-English definition
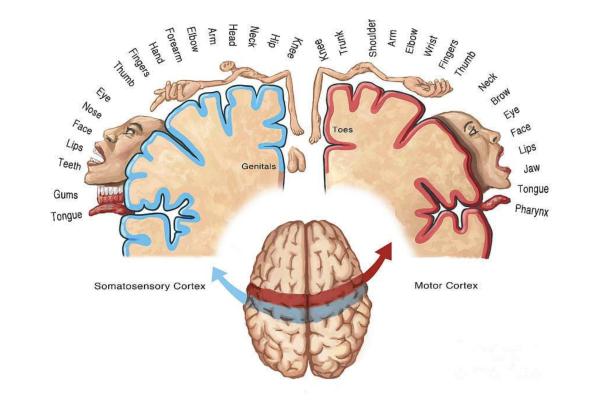
Penfield’s homunculus is a distorted body map drawn onto the brain’s surface that shows where each body part is represented for sensation (the sensory homunculus) and for movement (the motor homunculus). The map is “distorted” because it scales body parts not by physical size but by functional importance—how much detail or precision the brain needs for that region. That is why the lips, tongue, and hands appear enormous, while the torso and thighs are shrunken.
There are two companion maps. The sensory homunculus depicts how the brain “feels” the body—touch, vibration, and body position—while the motor homunculus depicts how the brain “does”—the outgoing commands that produce movement. Both maps are orderly (somatotopic), meaning neighboring areas on the body are represented by neighboring areas in the cortex, and both are contralateral: the left brain mostly maps sensations and commands for the right side of the body and vice versa.
Where the maps live: the brain’s two parallel strips
Imagine a headband of cortex arching from ear to ear, then focus on two parallel ridges split by a deep groove (the central sulcus). Just behind the groove sits the sensory strip (primary somatosensory cortex, S1), and just in front sits the motor strip (primary motor cortex, M1). The sensory strip belongs to the parietal lobe (postcentral gyrus), and the motor strip belongs to the frontal lobe (precentral gyrus). Each strip sweeps up and over the crown of the head and curves down the sides, continuing onto the brain’s inner wall toward the midline.
Within both strips, the body is laid out in a consistent sequence: face is represented more laterally near the temple; hand and arm lie more superiorly toward the top of the head; and leg and foot shift onto the brain’s inner (medial) surface. This “face-to-leg” progression is a hallmark of the homunculus and is clinically crucial for localizing symptoms.
How Penfield drew the homunculus: awake brain surgery and careful notes
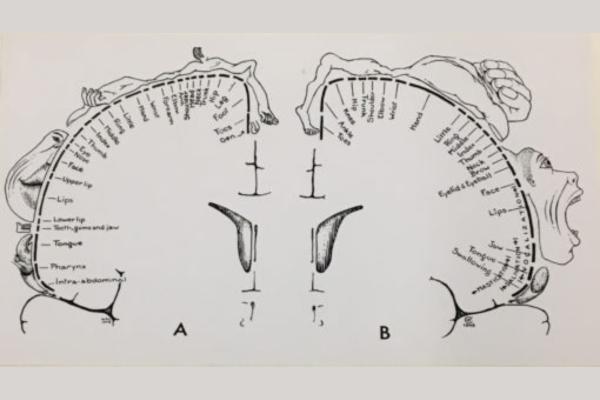
In the mid-20th century, Wilder Penfield and colleagues at the Montreal Neurological Institute developed an epilepsy surgery technique that kept patients awake and comfortable under local anesthesia. During the operation, they applied tiny electrical pulses to the exposed cortex and asked patients what they felt or observed what moved. When a specific spot on the sensory strip was stimulated, patients might report tingling on the thumb; a nearby spot might map to the index finger; a bit further along might produce sensation in the lips. Likewise, stimulating specific points on the motor strip could cause the mouth to twitch, fingers to flex, or toes to curl. By systematically plotting these responses onto the cortical surface, Penfield produced robust maps of sensory and motor representation—the homunculi we still use today.
Penfield emphasized that the drawings are summaries of many stimulation points—not perfect borders—but the big picture is remarkably stable across people. Later methods like functional MRI have refined the details, yet the core organization and the dramatic “magnification” of hands, lips, and tongue remain firmly supported.
Why the figure looks so strange: cortical magnification
The brain allocates neurons according to functional need, not body size. Areas packed with tactile receptors (like the fingertips and lips) or requiring fine, fractionated control (like the tongue and fingers for speech and grasping) get disproportionately more cortex. This principle is called cortical magnification. By contrast, the skin on the back or the large muscles of the thighs—needing coarse sensation and broad control—get less cortical territory. The homunculus scales each body part by its neural investment, hence the outsized hands and mouth and the minimized trunk and legs.
The sensory homunculus (S1): how the brain feels the body
The sensory homunculus lives in the postcentral gyrus. It builds a detailed moment-to-moment picture from bottom-up signals (touch, pressure, vibration, and proprioception—your sense of limb position). Neurons in fingertip regions have tiny “receptive fields,” meaning they respond to extremely small patches of skin, which supports exquisite discrimination of textures and edges. In contrast, neurons representing the mid-back respond to much larger patches of skin, so the sense of detail is blurrier there.
Two everyday demonstrations make this vivid. First, press two toothpicks a few millimeters apart on your fingertip—most people can feel two distinct points; try the same on your forearm or back and the points merge into one. That’s cortical magnification at work. Second, consider how much you can tell with your tongue about a single sesame seed in your mouth—that ultra-fine tactile sense reflects the massive representation of oral structures in S1.
Importantly, the sensory map is not static. With intense use, representational territory can expand; with disuse or injury, neighboring regions can encroach. Musicians, Braille readers, and craftspeople often show enhanced fingertip maps. After amputation, the region that once represented the missing part can be “invaded” by neighboring areas, contributing to phantom sensations when, for example, touching the face evokes a sensation in the absent hand (the face and hand are neighbors in S1).
The motor homunculus (M1): how the brain produces movement
The motor homunculus lives in the precentral gyrus. While early ideas imagined a one-muscle-one-spot code, modern evidence shows that M1 emphasizes coordinated movement patterns (synergies) and goals (e.g., grasping) rather than single muscle twitches alone. Regions controlling the hand, fingers, lips, and tongue occupy large swaths of cortex because they require precise, fractionated control—think playing a piano scale, typing, or articulating syllables rapidly.
Here too, plasticity matters. Skill training can strengthen or expand relevant territories, and focused rehabilitation after injury can help surviving regions take over lost functions. The map is a living blueprint shaped by practice and experience.
The somatotopic sequence: from face to leg along the strip
Both sensory and motor maps follow a consistent sequence in each hemisphere. Starting laterally near the temple, we find face, lips, and tongue. Moving upward along the strip leads to hand and fingers, then forearm and arm, and then toward the top and medial wall we find trunk, hip, leg, foot, and toes. The leg and foot representation dips onto the inner surface between the hemispheres.
This order is more than a diagram—it’s a clinical tool. If a person experiences sudden weakness or numbness primarily in the right face and hand, clinicians think about a lesion in the left lateral peri-Rolandic area (around the central sulcus); if the leg is disproportionately affected, the midline representation becomes suspect. The same logic helps explain the “Jacksonian march” in focal seizures: symptoms can spread in a sequence that mirrors the homunculus (thumb to hand to forearm to face), reflecting the spread of electrical activity across neighboring cortical territories.
How the maps guide clinical work
Penfield’s homunculi are not just teaching tools; they remain central to modern practice.
Diagnosis and localization: The face-hand-leg distribution helps clinicians localize strokes, tumors, and other lesions and predict which functions are at risk.
Neurosurgical mapping: In tumor and epilepsy surgery, teams often stimulate the cortex in real time to identify and preserve a patient’s specific motor and sensory regions, updating Penfield’s maps for that individual. This is a key reason awake craniotomy still matters—function is individualized, and borders can shift or overlap.
Seizure semiology: The homuncular sequence clarifies why tingling or clonic movements can “march” from one body part to the next during a seizure, guiding localization.
Rehabilitation: After stroke or nerve injury, task-specific, intensive practice (e.g., constraint-induced movement therapy for the hand) leverages plasticity to enlarge and strengthen relevant territories, improving function.
Brain–computer interfaces (BCIs): Modern systems decode intended hand movements from motor cortex signals to control robotic arms or cursors and, increasingly, deliver sensory feedback by stimulating the sensory strip. The homunculus is the roadmap for both decoding and feedback placement.

Why the mouth dominates: speech, feeding, and expression
Humans rely on extraordinarily precise lip, tongue, and jaw movements for speech and on fine oral sensation for feeding and social expression. The mouth’s dominance in both maps reflects high receptor density, rapid timing requirements, and the complex coordination needed for articulation and ingestion. This is why small disruptions in the lower face or tongue can have outsized effects on intelligibility and why infants explore their world by mouthing objects—the oral homunculus is richly endowed from the start.
What the homunculus is not: myths and misconceptions
“There’s a tiny person inside the brain.” The homunculus is a diagram, not a literal anatomical structure; it visualizes somatotopy (order) and magnification (priority) to make the invisible organization graspable.
“Each muscle has its exact spot.” The motor cortex encodes coordinated actions and patterns with overlapping territories; individual neurons can influence multiple muscles and joints.
“The maps never change.” Plasticity is the rule. Use, training, injury, and disuse reshape representational borders and strength; the overall scaffold persists, but details shift with experience.
“All pain lives in S1.” While the sensory strip helps locate and discriminate painful stimuli, the full experience of pain depends on broader networks (e.g., insula, cingulate), which encode affective and motivational dimensions.
Homunculi across species: form follows function
The same principles apply widely in mammals—but with species-specific distortions. Rodents exhibit “barrel cortex,” a specialized map for whiskers. Raccoons and primates show enlarged hand territories. Star-nosed moles devote huge cortical territory to their star-like nose rays. Where behavior requires precision and rich sensation, cortex invests. The rules of somatotopy and magnification transcend species.
Body illusions and the map you carry inside
The brain constructs body sense; it isn’t simply copied from the body. That’s why illusions teach us so much. In the classic rubber-hand illusion, synchronous stroking of a visible fake hand and a hidden real hand can shift feelings of ownership toward the fake hand. After amputation, touching the face can sometimes trigger sensations in the phantom hand, because facial inputs can “invade” the now-silent hand area in S1. These effects highlight that the homunculus is multisensory and plastic—shaped by the integration of vision, touch, and proprioception over time.
How to “feel” your homunculus at home
Try a few simple exercises:
Two-point discrimination: With eyes closed, gently touch the fingertip with two toothpicks a few millimeters apart; most people feel two distinct points. Repeat on the forearm or upper back; the two points blur to one. The difference reflects cortical magnification.
Texture ladder: Feel different textures (paper, denim, silk) with eyes closed using fingertip versus forearm; you’ll detect much finer differences via fingertip.
Motor individuation: Drum each finger in sequence (index to little and back). After a minute, speed improves—your motor map for those sequences is “warming up.”
Development, aging, and change across the lifespan
Early in life, neural connections are exuberant; practice and pruning refine the maps. Childhood skill learning (writing, playing instruments, sports) imprints durable sensorimotor patterns. With aging, some “dedifferentiation” can occur—borders become less crisp—but sustained engagement, practice, and health habits preserve function and can even sharpen representations. Across the lifespan, the principle holds: use it skillfully and you keep it; stop using it and neighboring functions take over.
Modern updates: networks, overlap, and individual variability
Penfield’s diagrams remain foundational, but modern neuroscience adds nuance. Sensation is distributed across S1, S2, insula, and cingulate; movement emerges from the interplay of M1, premotor cortex, supplementary motor area, basal ganglia, cerebellum, and parietal cortex. Territories overlap, borders are fuzzy, and individuals vary—shaped by genetics, learning, injury, and experience. That’s why clinicians still map function in real time during surgery; the homunculus gives the scaffold, and intraoperative testing fills in the particulars for each person.
Everyday takeaways: using the homunculus to live and work smarter
For skill building: Slow, precise, repeated practice changes the map; high-quality reps beat hasty volume. Musicians, surgeons, and athletes live by this.
For ergonomics: Tools that fit the hand’s functional anatomy harness the map’s precision and reduce strain. Fine work requires designs that respect fingertip sensitivity and joint mechanics.
For recovery: Task-specific therapy translates practice into cortical change; even modest daily routines compound over time.
For mind–body awareness: Jaw clenching, tongue posture, and shoulder tension are sensory “signals” you can adjust. Noticing and releasing micro-tensions taps directly into the sensory map and downshifts arousal.
Frequently made mistakes when thinking about the homunculus
Assuming size equals importance: On the homunculus, big means “precision and acuity,” not “strength.” The gluteus maximus is strong but gets modest cortical territory; the tongue is small but huge on the map because it must articulate and sense with astounding precision.
Confusing correlation with causation: Practice enlarges relevant representations, but more cortex is not always better; it’s better to aim for efficient, well-tuned maps than simply “bigger” ones.
Ignoring the network: S1 and M1 are critical nodes, but without premotor planning, cerebellar timing, and parietal guidance, movement and sensation are incomplete. The homunculus doesn’t act alone.
Why this still matters in the age of AI and neurotech
As brain–computer interfaces advance, the homunculus remains a practical targeting tool. Decoding intended hand or speech movements from motor cortex requires reliable access to hand and orofacial representations; evoking touch through sensory cortex requires stimulating the right somatotopic zones. The future of restorative neurotechnology is riding on principles Penfield sketched by hand: ordered maps, magnified priorities, and plasticity. Better imaging, smarter algorithms, and closed-loop feedback will refine these systems—but the homunculus remains the first map engineers and clinicians consult.
FAQs about Penfield’s Sensory and Motor Homunculus
What exactly is the homunculus in the brain?
It’s a distorted “little man” diagram drawn onto the sensory and motor strips that shows where each body part is represented for feeling and for movement, scaled by functional importance rather than size.
Where are the sensory and motor homunculi located?
The sensory homunculus sits in primary somatosensory cortex (postcentral gyrus), and the motor homunculus sits in primary motor cortex (precentral gyrus), on either side of the central sulcus.
Why do the hands, lips, and tongue look so big?
Because cortical magnification allocates more neurons to parts requiring fine sensation and precise control; high receptor density and demanding coordination inflate those regions on the map.
Are the maps the same for everyone?
The overall face-to-leg order and left–right (contralateral) organization are consistent, but borders and sizes vary across people and can change with use, practice, injury, or disuse.
How did Penfield create these maps?
During awake surgeries for epilepsy, he stimulated tiny cortical spots and recorded what patients felt (sensory) or what moved (motor), then plotted the results into orderly, reproducible maps.
Does the sensory homunculus include pain?
S1 helps localize and discriminate pain, but the full experience involves broader networks like the insula and cingulate; pain is not confined to a single “box” on S1.
Is the motor map one muscle per spot?
No—the motor cortex strongly encodes coordinated actions and patterns with overlapping territories; single neurons can influence multiple muscles and joints.
Why do some strokes cause isolated face or hand symptoms?
Because face and hand lie in specific lateral regions of the peri-Rolandic cortex; a small lesion there can impair those parts while sparing leg regions near the midline.
Can training change my homunculus?
Yes—focused, precise, repeated practice can strengthen or expand relevant representations in both sensory and motor cortex, improving skill and aiding recovery.
What is a quick way to experience the sensory map?
Try a two-point test: two toothpicks a few millimeters apart feel distinct on a fingertip but merge on the forearm—your sensory homunculus in action.
How does speech relate to the homunculus?
Face, lips, tongue, and jaw occupy large sensory and motor territories, supporting rapid articulation; higher-level language areas coordinate with these maps to produce fluent speech.
Why do surgeons still use these maps in the operating room?
They help localize and preserve critical motor and sensory regions during resections; surgeons often confirm the patient’s individual layout with real-time stimulation.
What’s the “Jacksonian march” and how does it relate?
It’s a seizure pattern where symptoms spread across body parts in the homuncular sequence (e.g., thumb → hand → arm → face), reflecting the brain’s orderly map.
Is the homunculus outdated in the era of brain imaging?
No—the homunculus remains the clearest entry point for understanding somatotopy; modern imaging adds nuance (overlap, networks, plasticity) without replacing the core map.
By citing this article, you acknowledge the original source and allow readers to access the full content.
PsychologyFor. (2025). What is Penfield’s Sensory and Motor Homunculus?. https://psychologyfor.com/what-is-penfields-sensory-and-motor-homunculus/